Introduction
Road traffic crashes are widely recognised as a significant global public health concern, leading to substantial fatalities and injuries (Singh & Singh, 2024). Globally, road traffic crashes are estimated to cause around 1.19 million deaths annually (WHO, 2023). In Iran, traffic crashes rank first in years of life lost due to premature death and second in overall causes of mortality. Approximately 2.5 percent of the world’s total traffic fatalities occur in Iran, a disproportionately high figure compared to global averages (Aghdam et al., 2024).
Pedestrians are one of the vulnerable groups in traffic crashes who are more at risk than other road users (Mwakalonge et al., 2015). Globally, pedestrians account for 22 percent and in some countries more than two-thirds of deaths due to road traffic crashes (Zegeer & Bushell, 2012). Among pedestrians, older adults are highly vulnerable (Sadeghi-Bazargani et al., 2018), due to age-related perceptual and cognitive deficits. These declines can affect their ability to perceive the road environment correctly, react in time, and process complex traffic situations (Jasiūnienė & Čygas, 2020; Pulvirenti et al., 2020).
Older adults are a part of society whose population, especially in developing countries such as Iran, is increasing significantly (Alipour et al., 2020; Sadeghi-Bazargani et al., 2018).
In Iran, studies show that the highest rate of road crashes in the older adult population involves pedestrians (Ghadirzadeh et al., 2012). The high rate of mortality of older pedestrians is observed in other countries besides Iran. People aged over 65 years old account for a third of pedestrian deaths in Australia (32%) (Gorrie et al., 2008) and in Ireland (36%) (Martin et al., 2010).
Several factors contribute to the increased traffic crashes among older pedestrians including declines in hearing and vision; reduced cognitive status, such as poor decision-making, difficulty in processing information, and difficulty in risk assessment (Zafar et al., 2014). Physiological conditions and limited physical abilities, skeletal, cardiovascular and neurological conditions that interfere with walking may also be involved (ErickTandi et al., 2019). Further, Liu and Tong (2014) reported that physiological changes in older adults due to aging and age-related complications contribute to their slower speeds in assessing risk and crossing the road, which puts them at a high risk of collision with vehicles.
Foundational work by Oxley et al. has further demonstrated that age-related declines in perceptual-motor and cognitive functioning significantly impact older pedestrians’ road-crossing decisions and safety, highlighting the need for age-specific considerations in traffic safety research (J. Oxley et al., 1997; J. A. Oxley et al., 2005).
One of the important factors affecting the performance of older adults is age-related cognitive decline. A common problem of ageing, cognitive decline can affect brain functions such as attention, memory, vision, reaction time, perception, judgment, reasoning, and problem-solving, most of which are necessary for safe pedestrian behaviour (Pavlou et al., 2017). Older adults can have poor performance in estimating the time of arrival of a car, and also decreased visual sensitivity, increased reaction time, and decreased speed of perception and processing which may increase the likelihood of a crash (Pavlou et al., 2017). A study of older adults conducted in 49 countries showed that functional and cognitive impairment is common among older adults in low-income countries (Lino et al., 2019).
While these functional declines increase the likelihood of crash involvement, the greater probability of serious injury or death among older adults primarily results from frailty (O’Hern et al., 2015). Frailty is a multidimensional syndrome characterised by a state of vulnerability, reduced multisystem physiological reserve, and decreased resistance to stressors (Panza et al., 2015). This physical fragility, along with cognitive function, can differ among individuals in this age group and significantly influence injury severity (Silva et al., 2023). This increased vulnerability means when involved in a crash, older pedestrians are at significant risk of injury or death (M. Guo et al., 2021).
Studies have shown that older pedestrians are particularly vulnerable in urban streets. This vulnerability may be attributed to factors such as reduced reaction speed and diminished confidence (D. Kim, 2019). Findings from a study conducted in East Azerbaijan, Iran, revealed that older individuals (aged >65 years) were involved in the majority of fatal vehicle-pedestrian crashes (60.8%), underscoring their heightened vulnerability. With the aging population growing and the significant risk of traffic crashes among older adults, the development of preventive initiatives for this group is imperative (Sadeghi-Bazargani et al., 2018). Moreover, traffic interventions aimed at improving pedestrian crossing behaviours are necessary (Bakhtari Aghdam et al., 2020). To assess the behaviour of older pedestrians and evaluate the impact of such interventions, an appropriate measurement tool is required.
Various questionnaires have been developed to assess pedestrian behaviour (Deb et al., 2017; Granié et al., 2013; McIlroy et al., 2019). These instruments typically evaluate pedestrian traffic behaviour across several domains, such as errors, mistakes, deliberate and unintentional violations, compliance with traffic regulations, behaviours associated with infractions, positive behaviours, distraction-related behaviours, and aggression or hostility in traffic settings. Despite the availability of these questionnaires, they are primarily designed for the general population. However, aging involves physiological and cognitive changes that significantly influence pedestrian behaviour in older adults (S. Kim & Ulfarsson, 2019) and none of these tools explicitly incorporate aging-related cognitive and perceptual declines or frailty-related physical limitations.
Previous research has demonstrated the necessity of age-specific assessment tools when evaluating various aspects of older adult health and behaviour. For instance, specialised questionnaires have been developed for measuring physical activity, quality of life, and lifestyle in older adults (Sandlin et al., 2014).
The originality of the current study lies in developing and validating the Older Adult Pedestrian Behaviour Questionnaire (OAPBQ) a culturally adapted, psychometrically tested instrument designed to capture the unique behavioural, cognitive, and physical dimensions of pedestrian safety among older adults. Unlike existing questionnaires, the OAPBQ incorporates domains such as Preference behaviours, reflecting compensatory adaptations linked to cognitive decline.
Moreover, this instrument establishes a foundation for future research integrating AI-based behavioural analytics and automated mobility systems. For example, it can be used in virtual reality or AI-assisted simulations to evaluate older pedestrians’ adaptive responses to emerging technologies such as automated vehicles, smart crosswalks, and connected transport infrastructure (X. Guo et al., 2023; Malik et al., 2024).
Given the absence of a standardised instrument for assessing pedestrian behaviour among older adults, this study aims to develop and validate a psychometric tool specifically tailored to capture the unique traffic behaviours and risk patterns of this demographic. The rationale for this study is grounded in the need to address the specific limitations of existing tools, which fail to account for age-related functional declines and the specific context of pedestrian safety in developing countries.
Methods
Study design and participants
This cross-sectional study was conducted from May 2023 to April 2024 in Tabriz, Iran, involving 600 people aged 60 years and older. A multistage sampling method was used. Initially, the city was stratified into four clusters based on socioeconomic status (West North, West South, East North, East South) (Jahangiry et al., 2020) and one healthcare centre (HCC) was randomly selected from each cluster (n = 4 HCC). The rationale for recruiting from HCCs is that the Iranian Integrated Health System (SIB) covers nearly the entire population, with over 98 percent of households registered at these centres; thus, this sampling frame ensures the sample is representative of the broader Tabriz population (Jahangiry et al., 2020).
Next, a list of households with registered individuals aged 60 years and older was obtained from the selected centres. Participants were then randomly selected from these households based on inclusion criteria and recruited from the four HCCs in two stages. First, participants (n = 300) completed the questionnaire for Exploratory Factor Analysis (EFA). Next, participants (n = 300) completed the questionnaire for Confirmatory Factor Analysis (CFA).
Sample size calculation
The sample size was determined based on a study by Jalilian et al. (Jalilian et al., 2015), considering a standard deviation (SD) of pedestrian behaviour scores (S = 3.25), a margin of error (d = 0.40), and a significance level (α = 0.05), resulting in an estimated sample size of 250. Given the cluster sampling method, the sample size was doubled to account for the design effect. Additionally, considering the likelihood of participant attrition among the older population, the final sample size was set at 600 individuals. The sample of 600 was randomly split into two equal subsamples (n=300 each) for EFA and CFA to provide independent datasets for model development and validation, a standard practice in psychometric research to avoid overfitting (Costello & Osborne, 2005). Demographic comparability between the two groups was assessed and confirmed prior to the factor analyses (see Results).
Inclusion and exclusion criteria
Participants were eligible for inclusion if they were: aged 60 years or older, able to walk independently without assistance (i.e., completely unaided, without the use of a walking stick, wheeled walker, motorised scooter, or help from another person), residents of Tabriz, willing to participate in the study.
Exclusion criteria were severe mental health condition (e.g., depression, Alzheimer’s disease, dementia), musculoskeletal disorders that restricted mobility, neurological impairments (e.g., stroke, Parkinson’s disease, paralysis), acute cardiovascular conditions (e.g., acute myocardial infarction, uncontrolled hypertension), severe hearing impairment or visual disturbances, incomplete questionnaire responses.
Selected participants were contacted via telephone, provided with information about the study, and invited to participate. Upon their visit to the healthcare centre, they received a detailed explanation of the study objectives, and informed consent was obtained before data collection.
Data collection instrument
Preliminary questionnaire and content validity assessment
The primary instrument used in this study was the 29-item Pedestrian Behaviour Questionnaire (PBQ), originally developed and validated for the general population by Bazargan et al. (2020). The Persian version of the PBQ used a 5-point Likert scale (1: Never to 5: Always) to evaluate pedestrian traffic behaviour across five domains:: 1. Compliance with traffic rules (7 items, e.g., For my safety, I cross behind a stationary truck or bus), 2. Violations and infractions (10 items, e.g., To save time, I cross intersections or streets diagonally), 3. Positive behaviours (6 items, e.g., I walk on the right side of the sidewalk to avoid disturbing other pedestrians), 4. Distracted behaviours (4 items, e.g., I use my mobile phone while crossing the street), 5. Aggressive behaviours (2 items, e.g., I get angry with other road users (drivers, pedestrians, cyclists) and insult them).
Additionally, a literature review was conducted to examine pedestrian behaviour measurement tools used in previous studies (Deb et al., 2017; Granié, 2009; McIlroy et al., 2019; Rezapur-Shahkolai et al., 2022; Vandroux et al., 2022).
Instrument development and content validity assessment
During the initial instrument-development stage, an expert panel of 15 professionals was assembled to guide item generation and content evaluation. The panel included specialists in traffic injury prevention, epidemiology, geriatric medicine, health education, traffic law enforcement, psychology, psychiatry, insurance, emergency response (Red Crescent, ambulance services), municipal planning, health workers, and senior health and traffic experts.
In this stage, seven new items were added to the questionnaire, expanding it to 36 items. The preliminary 36-item questionnaire was then sent to an expert panel for review, ensuring that the items were appropriate for the older population. Based on expert feedback, three additional items were incorporated, resulting in a 39-item questionnaire. These items emphasising age-specific challenges to reflect age-related cognitive, perceptual, and physical declines that influence pedestrian behaviour.
To qualitatively assess content validity, the revised 39-item questionnaire was resubmitted to the expert panel, who were asked to provide recommendations for improving, adding, or removing items to enhance the suitability of the questionnaire for older adults. Following the qualitative content validity assessment, some items were removed or merged based on expert feedback, resulting in a final 18-item questionnaire. The panel emphasised that reducing the number of items was essential to maintain participant engagement and ensure accurate responses. Expert panel members emphasised that existing pedestrian behaviour questions did not adequately reflect the cognitive, sensory, and physical changes common among older adults. To address this, new items were generated to capture difficulties with balance on uneven sidewalks, slower walking speed, divided attention in traffic, and inaccurate time-to-arrival estimation. For example, a Preferences item was introduced: “Because I cannot accurately estimate the time it takes for a vehicle to arrive, I choose safer (albeit longer) routes to cross the street.” This item and others were included in the draft questionnaire before content validity assessment and were subsequently evaluated by the panel.
For quantitative content validity assessment, the Content Validity Ratio (CVR) and Content Validity Index (CVI) were calculated. CVR was used to assess item necessity, while CVI measured item relevance. The questionnaire items were incorporated into a structured content validity form and re-evaluated by the expert panel. After aggregating the expert feedback, the questionnaire’s CVI (0.91), and CVR (0.82), indicated satisfactory content validity (Harlow et al., 2012).
Data collection
All 600 participants provided written informed consent before data collection. No participant withdrew or was excluded after consent; therefore, all 600 completed questionnaires were included in the analysis. Face-to-face interviews were conducted by a single trained researcher (the same researcher who performed all reliability assessments, described below) in a quiet, private room at the respective healthcare centre from which the participant had been recruited. Each interview lasted approximately 30 minutes. The researcher recorded responses directly onto a paper questionnaire form; these paper records were later double-entered into an electronic database by two independent data entry clerks to ensure accuracy. For the test-retest reliability assessment, a subsample of 30 participants completed the questionnaire a second time, following the identical procedure.
Reliability assessment
To evaluate the reliability of the instrument, test-retest reliability and Cronbach’s alpha coefficient were used. A sample of 30 older adult participants completed the questionnaire twice with a two-week interval. Questionnaires were administered in-person via face-to-face interviews, and all assessments were conducted by the same trained researcher to ensure consistency.
Exploratory Factor Analysis (EFA)
EFA was conducted to assess construct validity. The adequacy of the sample for factor analysis was evaluated using the Kaiser-Meyer-Olkin (KMO) test and Bartlett’s test of sphericity. Factors with eigenvalues equal to or greater than one was considered significant for extraction. Items with factor loadings of 0.4 or higher were retained, and principal component analysis (PCA) with varimax rotation was used for factor extraction.
Confirmatory Factor Analysis (CFA)
CFA was performed to assess how well the factor structure derived from EFA fit the data. Model fit was evaluated using the following fit indices, with their respective adequacy thresholds:
-
comparative Fit Index (CFI): > 0.80
-
Tucker-Lewis Index (TLI): > 0.80
-
root Mean Square Error of Approximation (RMSEA): Acceptable range: 0 to 1
-
standardised Root Mean Square Residual (SRMSR): Acceptable range: 0 to 1 (Bentler & Bonett, 1980; Kline, 2023)
Demographic and mobility variables
Six demographic variables were assessed in this study: age, gender, marital status, daily walking duration, education level, and the main transportation system used throughout the day (Bazargan et al., 2020). The daily walking duration variable was specifically included as a proxy for pedestrian exposure, allowing for an analysis of the relationship between the time spent walking and the frequency of specific pedestrian behaviours.
Data analysis
Data were analysed using SPSS (Version 25; SPSS Inc., Chicago, USA) and AMOS (Version 23.0; IBM Corp., Armonk, NY, USA). For quantitative variables, mean, SD, and median (Q1-Q3) were reported. For qualitative variables, frequency and percentage were calculated. The Kolmogorov-Smirnov test was used to assess data normality.
Results
Data were collected from a total of 600 participants aged 60 years and older, divided equally into two samples of 300 participants each for the EFA and CFA analyses. Among participants in the EFA sample, 124 (41.3%) were male and 176 (58.7%) were female, while in the CFA sample, 134 (44.7%) were male and 166 (55.3%) were female. The mean age of participants was 68.4 ± 6.2 years, with the majority belonging to the 60-70-year age group (EFA = 72.3%; CFA = 70.7%). In both groups, most participants were married (EFA = 83.3%; CFA = 75.0%), and a smaller proportion were divorced or widowed (EFA = 11.7%; CFA = 18.0%).
Regarding educational status, more than half of participants in both groups had no formal education (EFA = 62.0%; CFA = 57.3%), while a minority held a Bachelor’s degree or higher (EFA = 10.3%; CFA = 8.4%). In terms of daily walking duration, nearly half of the participants reported walking less than 30 minutes (EFA = 45.0%; CFA = 45.3%), while a smaller proportion walked more than two hours (EFA = 14.7%; CFA = 9.7%).
The main transportation mode reported was the personal car (EFA = 47.3%; CFA = 41.3%), followed by public transportation (EFA = 33.0%; CFA = 34.7%) and bicycle (EFA = 0%; CFA = 1.0%).
Comparative statistical analyses using chi-square and t-tests indicated no significant differences between the EFA and CFA samples across any demographic variable (p > 0.05), confirming that the two groups were demographically comparable and replicable (Table 1).
Exploratory Factor Analysis
The results indicated that the KMO test statistic was 0.58, suggesting an adequate sample size (Thanamee et al., 2017; Ussery et al., 2018). Bartlett’s test of sphericity was significant (χ² = 1394.27, p = 0.001), indicating intercorrelations among the variables (Beaudart et al., 2022). The principal component analysis identified four factors with a cumulative variance of 53.80 percent (p = 0.001).
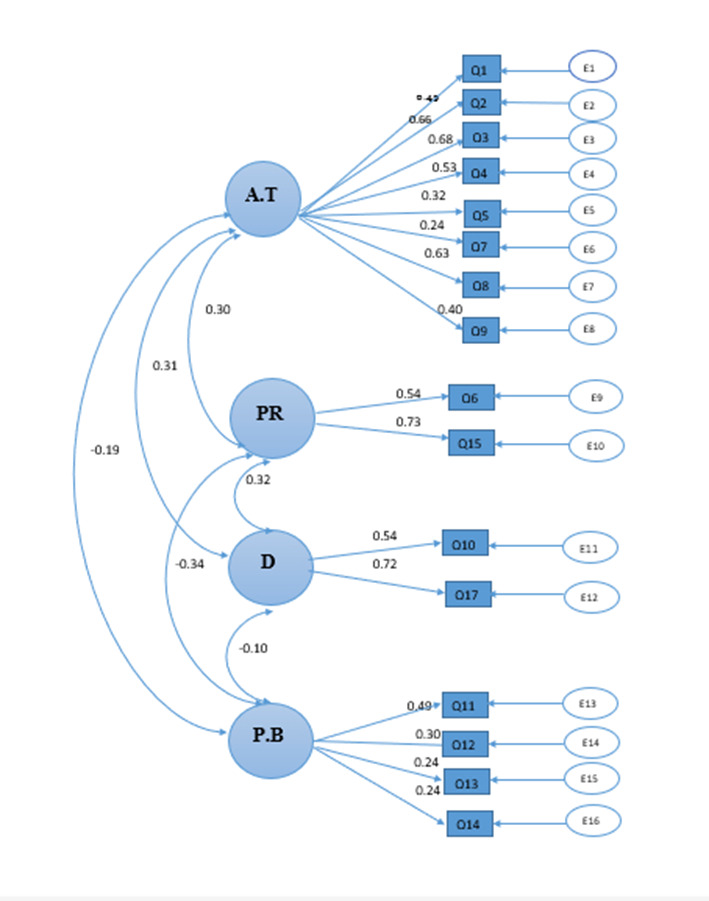
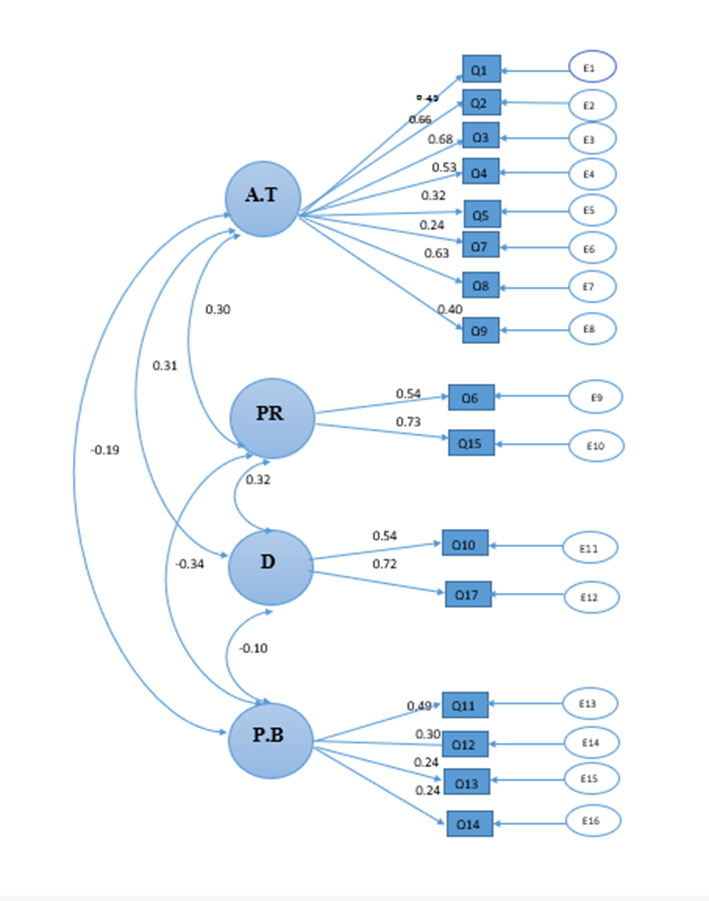
Table 2 presents the rotated factor loadings, where the factor loadings represent the correlation coefficients between each item and its corresponding factor. The identified factors were as follows: Factor 1 (Adherence to Traffic rules, 8 items), Factor 2 (Preferences, 2 items), Factor 3 (Distraction, 2 items), and Factor 4 (Positive Behaviours, 4 items).
The original PBQ included a Violation domain, which was merged with the Adherence to Traffic rules domain in the older adult population. Factor analysis results showed that older adults did not empirically distinguish between the two domains, which is consistent with earlier expert panel feedback that had suggested this might be the case.
The Distraction and Positive Behaviours domains were also present in the original PBQ and were retained in the OAPBQ, albeit with fewer items, based on the factor analysis results (items with loadings < 0.4 were excluded). Additionally, a new factor, Preferences (not present in the original PBQ), emerged from the EFA and met the same statistical criteria, justifying its inclusion. In the 18-item factor analysis, two items (Items 14 and 18) were removed due to low factor loadings, resulting in a final 16-item questionnaire. The complete list of items with their sources is provided in Appendix A.
Confirmatory Factor Analysis (CFA)
CFA was conducted on the final 16-item questionnaire to evaluate model fit using covariance matrices. All model fit indices demonstrated an acceptable level of goodness-of-fit, including the Goodness-of-Fit Index (GFI = 0.91), the Comparative Fit Index (CFI = 0.88), and the Root Mean Square Error of Approximation (RMSEA = 0.09). The GFI exceeded the conventional threshold of 0.90, indicating acceptable fit. The CFI approached the recommended criterion of 0.90, suggesting an adequate, though slightly suboptimal, fit. The RMSEA value of 0.09 is at the upper boundary of acceptable levels, typically interpreted as indicating a mediocre but still tolerable approximation error. Overall, the model demonstrated an acceptable fit to the data, supporting the factorial validity of the instrument for assessing pedestrian behaviour in older adults. Figure 1 presents the results of CFA for the OAPBQ.
Reliability Analysis
To evaluate the reliability of the instrument, both internal consistency and test-retest reliability were assessed. The internal consistency of the OAPBQ was examined using Cronbach’s alpha for both the EFA and CFA samples, as well as for the total sample. The overall Cronbach’s alpha coefficients were 0.539 for the first sample (EFA, n = 300), 0.469 for the second sample (CFA, n = 300), and 0.500 for the total sample (N = 600).
At the subscale level, the Adherence to Traffic Rules domain showed the highest internal consistency (EFA, α = 0.753; CFA, α = 0.671), followed by the ‘Preferences’ domain (EFA, α = 0.552; CFA, α = 0.541). The Positive Behaviours (EFA, α = 0.36; CFA, α = 0.35) and Distraction domains (EFA, α = 0.06; CFA, α = 0.08) demonstrated lower reliability values, which may be due to the small number of items and greater behavioural variability among older adult participants.
Despite the modest overall alpha coefficients, the factor structure confirmed by CFA provide some supports for the multidimensional construct validity of the OAPBQ. However, the Cronbach’s alpha values for the Distraction (α = 0.06–0.08), Positive Behaviours (α = 0.34–0.36), and Preferences (α ≈ 0.55) subscales were below the commonly accepted threshold of 0.70, indicating poor internal consistency for these subscales.
Table 3 presents the Cronbach’s alpha coefficients for each domain across the two samples and the total sample.
Test-retest reliability demonstrated an excellent level of temporal stability, with r = 0.89 and rSB = 2r/1-r = 0.94. These values are consistent with prior findings reported in similar behavioural measurement instruments (Rezaei et al., 2023).
The standardised mean (SD) traffic behaviour score of older pedestrians in this study was 78.85 (6.94). Among the four behavioural dimensions, the highest score was observed in the Preferences domain, suggesting that older pedestrians exhibited cautious behaviours. The lowest score was recorded in the Distraction domain, indicating higher levels of distraction among older pedestrians in traffic environments. Table 4 presents the mean and median scores for the different domains of the OAPBQ.
These findings provide a structured understanding of older adult pedestrian behaviours, emphasising their cautious tendencies and susceptibility to distraction in traffic environments.
Discussion
The primary objective of the present study was to develop an adapted version of Pedestrian Behaviour Questionnaire (PBQ) suitable for use with older adults, and to assess its reliability and validity. This 16-item questionnaire categorises older pedestrian behaviours into four domains: 1) adherence to traffic rules, 2) positive behaviours, 3) distraction, and 4) preferences. The overall Cronbach’s alpha for the OAPBQ was 0.50, which is below the conventional threshold of 0.70 and does not confirm reliability. In comparison, previous studies using the PBQ in the general population have reported alpha values above 0.70 (Deb et al., 2017: above 0.70; Bazargan et al., 2020: 0.84; Rezapur-Shahkolai et al., 2022: 0.89). The lower reliability coefficient observed in the current study may be attributed to differences between older adults and the general population, but it is also likely a consequence of the small number of items in certain subscales and the expert-driven item reduction prior to factor analysis. The reduction, although necessary for content validity, may have limited the pool of items available for statistical selection and thus could have contributed to the lower alpha values in some subscales. Future studies may consider starting with a larger item pool to allow greater statistical reduction. Moreover, the instrument was deliberately kept short (16 items) upon expert panel advice to reduce respondent burden and encourage completion among older adults; while this improved feasibility, it further limited the number of indicators per factor, which likely also contributed to the low alpha values.
However, when examined separately, the Adherence to Traffic Rules domain showed the highest internal consistency (α = 0.72). In contrast, Cronbach’s alpha values for the Distraction (α = 0.06–0.08), Positive Behaviours (α = 0.34–0.36), and Preferences (α ≈ 0.55) subscales were unacceptably low and fell well below the conventional threshold of 0.70. These low values are likely attributable to the very small number of items per subscale and the high behavioural variability among older adults (Tavakol & Dennick, 2011). Consequently, scores on these three subscales should be interpreted with extreme caution, and further refinement, particularly the addition of more items to these domains, is strongly recommended before the OAPBQ is used for individual assessment or decision making.
Nevertheless, the test-retest reliability was excellent, confirming the temporal stability of the OAPBQ over time. This pattern, modest to low internal consistency alongside strong temporal reliability, has been observed in other behavioural tools for older adults (Agarwal et al., 2019). Therefore, while internal homogeneity across items is modest, the instrument reliably measures stable behavioural tendencies among older pedestrians.
From a psychometric perspective, future studies could employ composite reliability or McDonald’s omega, which are less sensitive to the number of items than Cronbach’s alpha and may provide a more accurate estimation of reliability in multidimensional scales (Hayes & Coutts, 2020). Additionally, refining or expanding the lower-performing subscales may further enhance internal consistency in future versions.
To assess the validity of the OAPBQ, both content analysis and factor analysis were employed. Expert panel members emphasised that certain questions included in general traffic behaviour questionnaires were not suitable for the older adult population. This judgment was grounded in evidence that age-related declines in cognitive and perceptual function (De Vito et al., 2025; S. Kim & Ulfarsson, 2019) and reduced ability in time estimation and divided attention (Shi et al., 2020) alter the way older adults interact with traffic. Consequently, several items were modified or adjusted based on expert feedback. Additionally, a new domain, preferences, was introduced, while the aggressive behaviour domain was omitted. The difference in the number of domains between the OAPBQ (four domains) and the PBQ (five domains) is likely due to the differences in target populations. Furthermore, the OAPBQ contains fewer items (16) than the PBQ (29), a design choice made to accommodate the needs of older participants. OAPBQ values for CVI (0.91) and CVR (0.82) indicate a satisfactory level of content validity. In contrast, the content validity values for the Iranian PBQ in the general population (CVI: 0.86; CVR: 0.88) (Bazargan et al., 2020). The slightly higher CVI and comparable CVR for the OAPBQ indicate that the adapted items were at least as relevant and necessary for older adults as the original items were for the general population, confirming that the expert-driven modifications successfully aligned the instrument with the target age group’s characteristics.
Factor analysis results identified four domains in the OAPBQ, consistent with a study by Rezapur-Shahkolai et al. (2022), which also identified four domains for measuring adolescent pedestrian behaviour: unsafe road-crossing behaviour, distraction, positive behaviour, and playing on the road. Notably, the distraction and positive behaviour domains were similar across both instruments. The differences in the remaining two domains can be attributed to the characteristics of the respective target populations. Given the physiological changes associated with aging, older adults tend to adopt more cautious behaviours and prioritise options that minimise their risk of harm. In contrast, behaviours such as playing on the road are relevant to children and adolescents but not to older adults.
In addition to the Preference items, other modifications to the OAPBQ were made to better reflect cognitive, sensory, and attentional changes common among older adults. For example, items addressing Distraction and Positive Behaviours were refined to capture realistic age-related limitations such as reduced working memory, slower reaction time, and compensatory strategies (e.g., avoiding multitasking while crossing). These revisions align with previous findings that age-related cognitive decline affects situational awareness and attentional allocation during walking (De Vito et al., 2025). Moreover, older adult participants in this study demonstrated lower scores in the distraction subscale and higher scores in the preference subscale, suggesting that while cognitive decline may impair divided attention, older adults compensate through cautious decision-making and risk-avoidant behaviour. This nuanced pattern supports the ecological validity of the OAPBQ in capturing real-world adaptations among older pedestrians.
In the OAPBQ, one of the preference items highlights the presence of environmental obstacles on sidewalks, such as potholes, which can increase the risk of falls, a significant concern for older adults. This aligns with findings by McIlroy et al. (2019), who emphasised the crucial role of the physical environment in shaping pedestrian behaviour, particularly for individuals with special needs, including older adults and people with a physical disability.
Previous studies assessed pedestrian behaviour in the general population across five domains (Antić et al., 2016; Deb et al., 2017; McIlroy et al., 2019; Sadeghi-Bazargani et al., 2018). In contrast, the present study measured older pedestrian behaviour across four domains. Three domains, Distraction, Adherence to Traffic Rules and Positive Behaviours, align with the Iranian PBQ. However, panel members in the current study noted that the adherence and violation domains in the PBQ overlapped, making it difficult for older respondents to distinguish between them. They argued that violation inherently involves Adherence to Traffic rules, leading to the merging of these two domains. While violation is included in various international pedestrian behaviour questionnaires, adherence is unique to the Iranian PBQ (Sadeghi-Bazargani et al., 2018). Furthermore, the results of both the EFA and the CFA demonstrated a stable four-factor structure with acceptable model fit indices. The absence of significant demographic differences between the EFA and CFA samples confirmed that the two groups were comparable and replicable, supporting the generalisability of the findings. Together, these results provide empirical evidence for the structural validity of the OAPBQ and demonstrate that its four domains capture distinct yet interrelated dimensions of older adult pedestrian behaviour.
The coherence between the EFA and CFA findings also supports the view that differences from previous scales are not merely population effects but represent reasoned psychometric refinements. For example, merging the adherence and violation domains was empirically supported by factor loadings, while the emergence of the preference domain highlights behavioural adaptations specific to older adults. These findings provide preliminary support for the conceptual structure of the OAPBQ and its replicability across independent samples (Kline, 2023). However, given the low internal consistency of several subscales and the overall modest reliability indicate that the instrument requires substantial further development. Consequently, the OAPBQ offers a tentative sound framework for describing older adult pedestrian behaviour and more work is needed to strengthen its psychometric properties before it can be recommended for applied use.
Another key difference between the OAPBQ and the Iranian PBQ (Sadeghi-Bazargani et al., 2018) is the handling of the aggressive behaviour domain. In the OAPBQ, aggressive behaviour items were incorporated into the Adherence to Traffic rules domain, which is theoretically justifiable. For example, striking a vehicle out of anger constitutes a form of traffic rule violation. Moreover, previous studies using the PBQ, older adult populations have shown that older adults exhibit lower aggressive behaviour scores compared to other domains (i.e., Adherence to Traffic Rules, Positive Behaviours, and Distraction); for example, aggressive behaviour scores have been found to be lower than adherence scores (Aghdam et al., 2024). Similarly, other research has indicated that aggressive behaviour scores among older adult individuals are lower compared to younger age groups (M. Liu et al., 2021)
As a result, the Preference domain emerged in the factor analysis of the OAPBQ. This domain includes two items, one of which states: ‘Because I cannot accurately estimate the time it takes for a vehicle to arrive, I choose safer (albeit longer) routes to cross the street.’ This finding is theoretically plausible, as a study by Shi et al. (2020) demonstrated that older adults who struggle with time estimation are at a higher risk of traffic-related injuries. Several other items were adapted or developed to capture age-related perceptual and physical changes. For example, questions were included to assess difficulties in maintaining balance on uneven sidewalks, reduced walking speed when crossing streets, and the influence of divided attention when navigating complex traffic environments. Although some of these items were excluded during factor analysis due to low loading values, their initial inclusion was instrumental in refining the construct of the Preference and Distraction domains. Importantly, the older adults showed higher mean scores on the Preference items compared to the other OAPBQ subscales, supporting the notion that older adults compensate for cognitive and perceptual decline through more cautious and risk-avoidant strategies (De Vito et al., 2025). These findings expand our understanding of how aging-specific cognitive and sensory challenges shape pedestrian decision-making behaviours. Also, cognitive and perceptual function decline in older adult individuals may necessitate alternative strategies for tasks requiring rapid and precise responses, such as crossing busy streets (S. Kim & Ulfarsson, 2019).
O’Hern et al. (2020) developed a 32-item questionnaire for individuals aged 18-65 years, categorising pedestrian behaviour into four domains: violations, errors, aggression, and technology engagement. Similarly, Granié et al. (2013) developed a 23-item questionnaire assessing pedestrian behaviour across four domains: transgression, lapses, positive behaviours, and aggressive behaviours in a population aged 15-78 years. Notably, Granié et al. identified age-related differences in behavioural dimensions, such as a decrease in violations with age, which provides useful context for understanding the distinct behavioural patterns of older adults. While these instruments share a structural similarity with the OAPBQ, the OAPBQ is distinct in that it is specifically adapted to address the unique perceptual and cognitive needs of the older adult population (60+ years). Overall, the findings provide some initial support for the validity of the OAPBQ; however, given the low internal consistency of several subscales, further refinement of the instrument is necessary before it can be considered suitable for widespread use in assessing older pedestrian behaviour.
Study strengths and limitations
This is the first instrument developed and validated for assessing older pedestrians in Iran; cross-cultural validation is needed for use in other countries. A robust psychometric evaluation was conducted, including both exploratory and confirmatory factor analyses on separate samples. This study has several limitations that warrant consideration. First, a significant portion of the participants, approximately 60 percent, were illiterate, and many experienced age-related cognitive or physical impairments that hindered their ability to complete the questionnaire independently. As a result, the researcher frequently provided assistance in administering the instrument, which may have introduced a degree of interviewer bias or inadvertently influenced participant responses. Second, the internal consistency of the instrument, as measured by Cronbach’s alpha, was below the generally accepted threshold of 0.70 for the overall scale and several subscales. This may be attributable to the low number of items in certain domains; future research should focus on adding or refining items to enhance the reliability of the OAPBQ. Third, the study sample was drawn exclusively from older residents in Tabriz, potentially limiting the generalisability of the findings to broader or more diverse older adult populations, thus requiring careful interpretation when extending the results beyond this context. To enhance the generalisability of the findings, future studies should assess the psychometric properties of the OAPBQ across diverse geographic and cultural settings within Iran. Evaluating the tool in varied provincial contexts will help determine its robustness and applicability across different older adult populations. Furthermore, given the current lack of a standardised international instrument for assessing pedestrian behaviour in older adults, it is recommended that the questionnaire be translated into English and subjected to cross-cultural validation. Such efforts would facilitate international comparisons and contribute to the global literature on older adult pedestrian safety and behaviour assessment.
Conclusion
This study presents the development and psychometric validation of a novel instrument designed to assess traffic-related behaviour among older pedestrians. The questionnaire demonstrated acceptable validity, offering a contextually relevant and methodologically sound tool for evaluating behavioural patterns that may influence traffic safety in older adults. However, the internal consistency of the scale was modest, indicating a need for further research to refine the items and improve the reliability of the measure. Given the vulnerability of this population in traffic environments and the lack of existing standardised measures, the OAPBQ addresses a critical gap in the field. While the findings are promising, further validation across diverse settings and populations is essential to strengthen the instrument’s generalisability and support its broader application in public health interventions, urban planning, and road safety policymaking targeting older adult populations.
AI tools
ChatGPT 4 was used for English expression and clarity.
Acknowledgements
The authors would like to acknowledge all the participants for their contribution to the present study.
Author contributions
FBA and HSB wrote the first draft. AJK, SS, and LJ were involved in the data collection and data analyses. PH restructured and rewrote the first draft. All authors reviewed the final version of the manuscript.
Funding
Tabriz University of Medical Sciences provided funding sources for this study. Study collaborators were all employees of Tabriz University of Medical Sciences at the time of study conduct. The findings and conclusions in this paper are those of the authors and do not represent the views of the Tabriz University of Medical Sciences. The funding body had no role in the design of the study and collection, analysis, interpretation of the data, writing the manuscript, and publication as well.
Human research ethics review
All subjects gave their informed consent for inclusion before they participated in the study. The protocol was approved by the Ethics Committee of Tabriz University of Medical Sciences (Approval Code: IR.TBZMED.REC.1401.758).
Data availability statement
Data used for this project are available with researcher ethics approval from the corresponding author.
Conflicts of interest
The authors declares that there are no conflicts of interest.