Introduction
Access to information and support is essential to ensure safe transport for all children, including those with disabilities and medical conditions. The correct use of appropriate car seating systems and restraints is critical to the safety of children during road transport and is mandated by Australian laws and standards. Despite these requirements, road vehicle crashes remain a leading cause of death for children both in Australia and internationally (AIHW, 2024; WHO, 2023).
Disabilities (including diagnosed developmental, cognitive, or physical conditions that interfere with functioning,), medical conditions, and physical injuries can impact the road safety transport of children. Children with disabilities and medical conditions face an even greater risk of injury or death in the event of a crash, yet these children have received relatively little attention in transportation research compared to other populations (Downie et al., 2020). Children with disabilities and medical conditions may have additional car seating needs that are not addressed by common and commercially available car seating and restraint systems, rendering these systems ineffectual in protecting the child. These needs may be due to physical differences (e.g., posture, movement) that require specially designed car seats or from medical conditions that require equipment to be transported with the child (Downie et al., 2020; Yonkman et al., 2010). At the same time, children with various neurodevelopmental conditions may experience significant distress during road transport due to unique psychological and sensory needs, which can lead to concerns about their attempts to leave the car seat or exit the vehicle (Black et al., 2023; Plummer et al., 2021; Yonkman et al., 2013). In these cases, specialised car seating and restraint systems or modifications are required to improve the comfort and safety of the child (Cook, Brown, et al., 2024; Downie et al., 2020).
For children with disabilities and medical conditions, a ‘one-size fits all’ approach is rarely effective, and specialised car seating systems, modifications, and behavioural strategies may be implemented depending on the child’s unique needs. Health professionals and organisations play a vital role in ensuring that children with disabilities and medical conditions are provided with safe, effective, and appropriate seating and car restraint systems. In Australia, the standard Child Restraint Systems for Use in Motor Vehicles (AS/NZS 1754:2013) includes minimum design, construction and performance requirements. However, there are no such requirements in the standard Restraint of Children with Disabilities, or Medical Conditions, in Motor Vehicles (AS/NZS 4370:2013) that provides health professionals with some guidance on prescribing car seating systems for children with disabilities and medical conditions (Standards Australia, 2013). Instead, AS/NZS 4370 promotes modifications of child restraint systems without evidence of their impact on restraint effectiveness and puts children at risk of injury (Cook, Whyte, et al., 2024). The lack of equivalent in-vehicle safety protection for children with disabilities and medical conditions has resulted in an overreliance on health professionals’ clinical reasoning when working with caregivers and children to identify supports, products and strategies.
In 2020, a survey of Australian health professionals and organisations that support the transport needs of children with disabilities and medical conditions, highlighted critical concerns about their perceived ability to ensure safe transport for these children (Black et al., 2024). Health professionals and organisations reported various challenges, most prominent were a lack of appropriate knowledge, support and training (Black et al., 2024). Findings from the 2020 survey identified an immediate need for action to improve access to training and resources, and to improve knowledge and confidence of health professionals and stakeholders.
The findings of this study and others (Black et al., 2024; Cook, Brown, et al., 2024) prompted Mobility and Accessibility for Children and Adults Ltd (MACA) to optimise their information and develop training courses. Since 2020, MACA provided targeted information and training resources via an online platform (https://www.macahub.org). MACA has developed specific resources for parents, allied health professionals, disability product suppliers and other stakeholders. Resources include a website, specialist training courses, an expert support service and a portal with prescribing resources for trained professionals. The information covers the topic areas of products, road laws, policies, transport challenges, research projects and parent stories.
However, the impact of these resources on road safety practices in Australia is unknown. Therefore, the aims of this study were to: a) understand the current experiences and perspectives of health professionals and organisations; b) identify any changes in these experiences and perspectives since 2020; and c) explore the use and perceived helpfulness of MACA resources for health professionals and organisations supporting the safe transport of children with disabilities and medical conditions.
Method
Design
This study was a national online survey to assess the safe transport practices for children with disabilities and medical conditions in Australia. We include children with disabilities and children with medical conditions, as both face transport safety challenges. In Australia, children with disabilities and medical conditions are included in the same standard, Restraint of Children with Disabilities, or Medical Conditions, in Motor Vehicles (AS/NZS 4370:2013). The same survey used in 2020 (Black et al., 2024) was administered to three key stakeholder groups: health professionals who provide support for safe transport, representatives from transport-related organisations, and caregivers of children with disabilities and medical conditions. This paper presents the quantitative findings from the health professionals and organisational representatives.
Materials
The survey tool from Black et al. (2024) was utilised. It primarily consisted of quantitative questions, including multiple choice (multiple and single answer), and Likert scales (1-10 with 10 the highest score). Survey questions were tailored to the different stakeholder groups. For professionals, questions included demographics (e.g., practice area, background), assessment practices, knowledge and beliefs, challenges in addressing transport needs and accessing information. For organisations, questions included demographics (e.g., organisation type, size), knowledge and beliefs, plans and strategies and involvement in research related to transport of children with disabilities and medical conditions. In addition to the 2020 survey questions, participants were also asked about their knowledge and use of MACA resources, and their perceived helpfulness in supporting the safe transport of children with disabilities and medical conditions. The survey was created and administered using Qualtrics.
Recruitment
Participants of the 2020 survey who had consented to be contacted were invited to repeat the survey. Additionally, participants were recruited through disability service organisations and advocacy groups, including via newsletters, emails and social media posts. Participants were provided with information about the study and gave informed consent (within the survey platform) prior to commencing the survey. Incentives were used to encourage participation. Respondents who completed the full survey were invited to enter a raffle for one of three $50 gift vouchers as an acknowledgement of their time.
Statistical analysis
Data were analysed using IBM SPSS Statistics (version 30.0.0.0). Data were cleaned, including the removal of ineligible responses (<50% of questions answered). Variables were analysed descriptively, including counts, percentages, means and standard deviations. For Likert scale data, medians and interquartile ranges (IQR) were used as measures of central tendency and data variability. Health professionals and organisations were analysed separately.
After the analysis of the 2023 data, variables were compared with the 2020 dataset (Black et al., 2024), with changes between the two time points described using counts and percentages. Additionally, participants who responded to both surveys (repeat participants) were analysed as a subgroup, to explore changes over time. To identify if the repeat participant sub-group was a demographically similar group to the total sample, a chi-squared test was conducted to compare the frequency of health professional make-up, and time-spent practising in their profession; while a Fisher’s Exact chi-squared variation was used to check for differences between work settings and common disabilities or medical conditions treated. These changes were explored using percentages, with McNemar’s test (for dichotomous data) and the Wilcoxon signed ranks test (Z) used to identify statistically significant changes between the two timepoints.
Results
Sample
A total of 177 individuals responded to the survey (health professionals, n=136; organisational representatives, n=41) and 11 incomplete surveys were excluded. A total of 166 responses (health professionals, n=126; organisational representatives, n=40) were included in the analysis. Of these respondents, repeat participants were both health professionals (n=56, 44.4%) organisational representatives (n=18, 45.0%).
In the 2023 sample, health professionals (n=126) were mostly occupational therapists (n=97, 77.0%) or physiotherapists (n=21, 16.7%) and most had more than ten years of experience (n=83, 65.9%). Among all health professionals, most worked at not-for-profit organisations (n=34, 27.0%) or private group practices (n=34, 27.0%), followed by hospital settings (n=22, 17.5%) and sole provider private practices (n=21, 16.7%). Health professionals provided transport assessment services primarily for clients with cerebral palsy (n=86, 70.6%), autism (n=62, 51.6%), global developmental delay/intellectual disability (n=49, 40.5%), and neurological conditions (n=43, 34.1%). Health professionals from all states within Australia were represented in the survey with the greatest representation from Victoria (n=38, 30.2%) and New South Wales (n=32, 25.4%) with a mean Index of Relative Socio-Economic Advantage and Disadvantage of 6.1 (± 2.7) (Walker & Hiller, 2005).
The professions of the repeat participant subgroup were similar to the total 2023 sample (occupational therapists; n=44, 78.6% and physiotherapists: n=9, 16.1%) and had similar experience (10+ years: n=41, 73.2%). More of the repeat participants worked in private group practice (n=18, 32.1%) than not-for-profit organisations (n=12, 21.4%) while a similar proportion worked in sole provider private practice (n=12, 21.4%) and hospital settings (n=10, 17.9%). Disability among the clientele of repeat participants was also similar to the total 2023 sample. The majority of health professionals provided transport assessment services for clients with cerebral palsy (n=43, 76.8%), autism (n=25, 44.6%), global developmental delay/intellectual disability (n=23, 41.1%) and neurological conditions (n=23, 41.1%). Repeated sample health professionals were from all Australian states and territories. Once again, the states with greatest representation were Victoria (n=17, 30.3%) and New South Wales (n=16, 28.5%).
Descriptive and demographic information also shows that the repeat sample was similar to the one-time respondents in the 2020 sample (Black et al., 2024). In 2020 a similar percentage of respondents were occupational therapists (n=153, 65.4%) and physiotherapists (n=29, 12.4%). A The largest proportion of practitioners had more than 10 years of experience (n=102, 43.6%) which is to be expected as this survey was conducted three years prior. A similarly large proportion of participants worked in not-for-profit organisations (n=75, 29.6%) but a lower proportion worked in private group practices (n=47, 18.6%). Health professionals in 2020 also supported fewer clients with cerebral palsy (n=43, 76.8%), autism (n=25, 44.6%), global developmental delay/intellectual disability (n=23, 41.1%) and neurological conditions (n=23, 41.1%). A range of organisations were represented within the 40 organisational representatives who participated, including health (n=9, 22.5%), transport (n=7, 17.5%), disability (n=6, 15%), education (n=6, 15%), as well as product suppliers, manufacturers, and installers (n=6, 15%). The only significant demographic differences existed in the years that repeat respondents had spent practising compared to one-time respondents. The number of repeat respondents that reported practising for 5-10 years and 10+ years was significantly greater (Χ2 = 8.48, p = 0.04) than the one-time respondent cohort. A limitation of the repeat respondent cohort is due to selection bias because repeat respondents needed to have been practising for at least four years to complete both surveys. This selection bias limits the generalisability of repeat respondent findings to practitioners with less than four years’ experience.
Health professional assessment recommendations and prescription practices
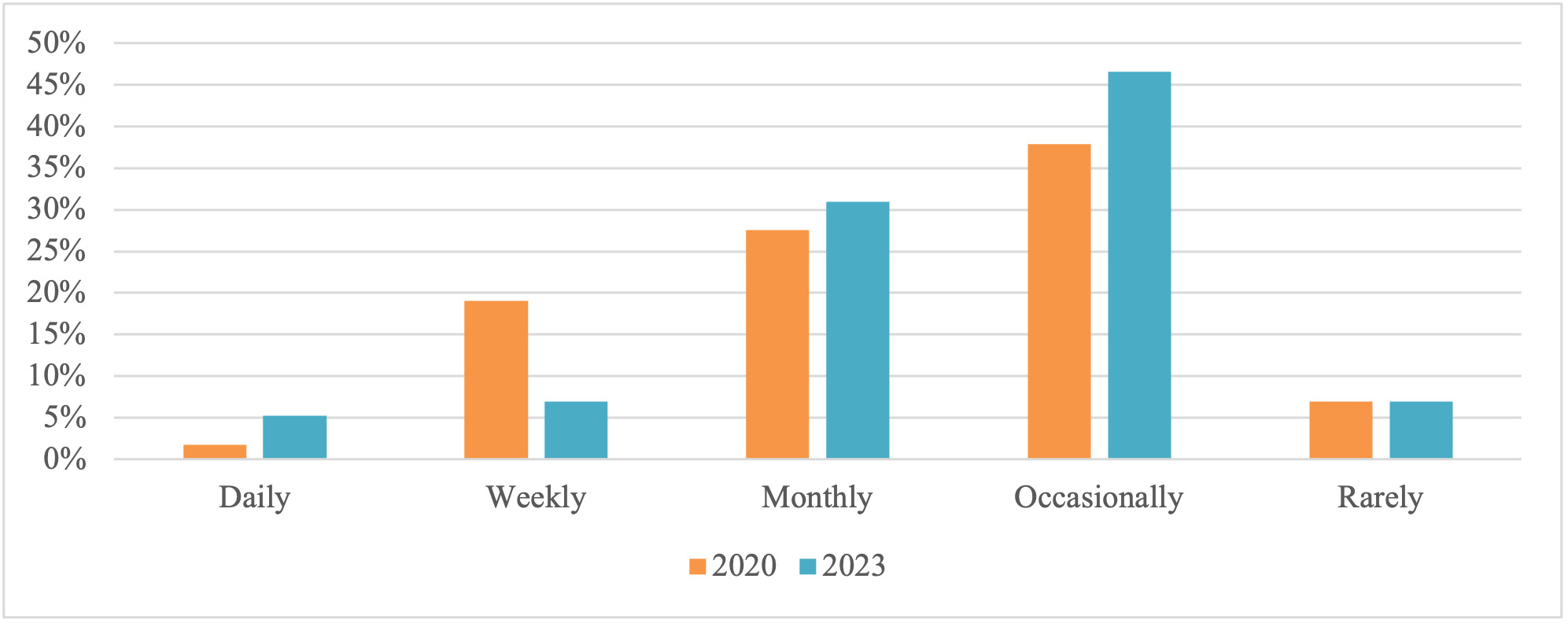
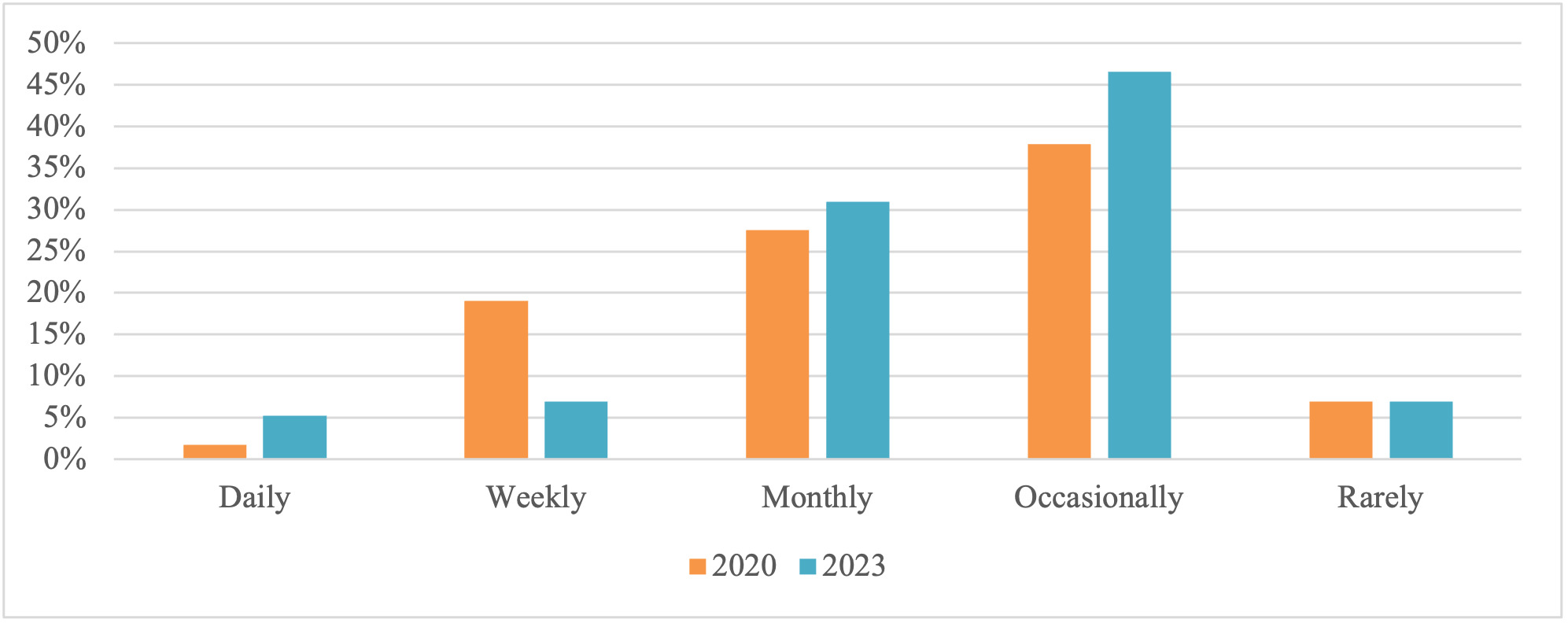
Health professionals most frequently reported they addressed the transport needs of their clients ‘occasionally’ (1-2 times per year, n=57, 45.2%) or ‘monthly’ (n=44, 34.9%). Only 16 participants reported providing these services more frequently (weekly: n=12, 9.50%; daily: n=5, 4.0%). Eight participants (6.3%) reported rarely addressing car seating and transport needs for children with disabilities or medical conditions. When examining repeat participants between the 2020 and 2023 time-points there was a modest increase in health professionals addressing their clients’ transport needs daily and monthly, but a decrease in those doing so weekly (Figure 1).
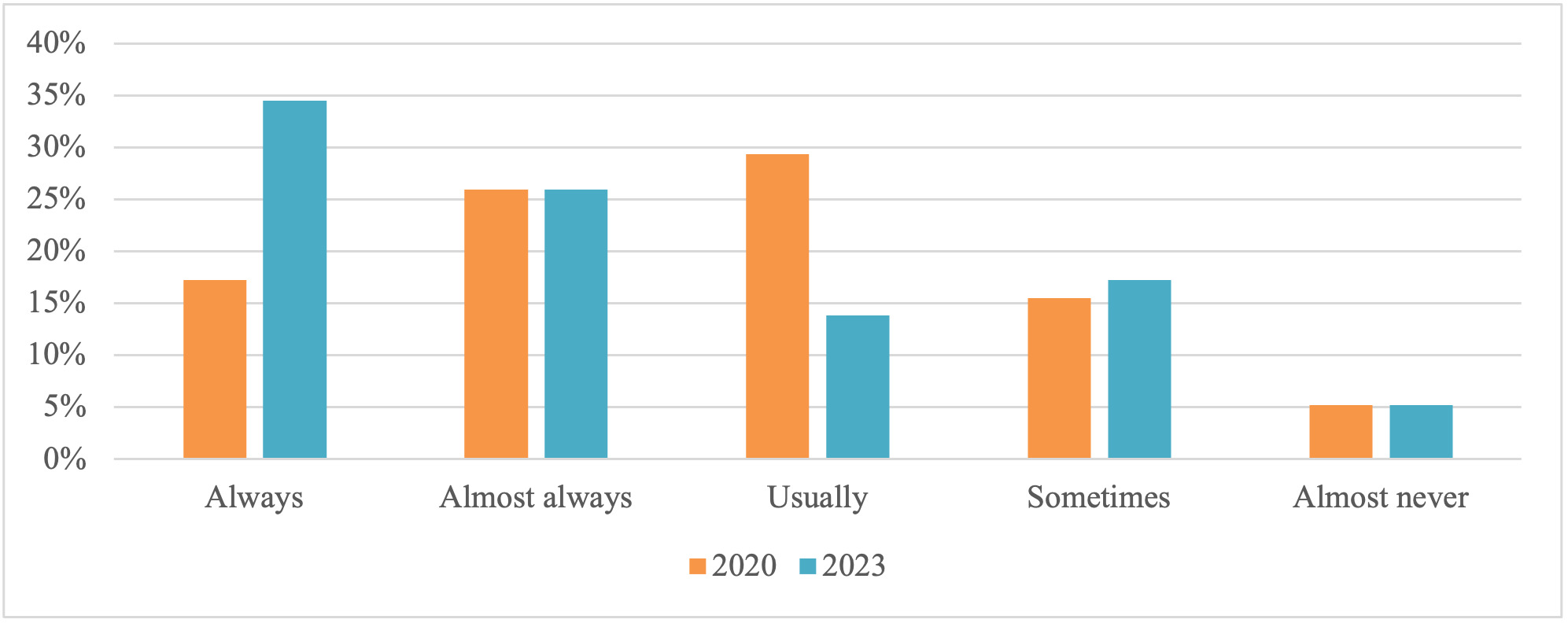
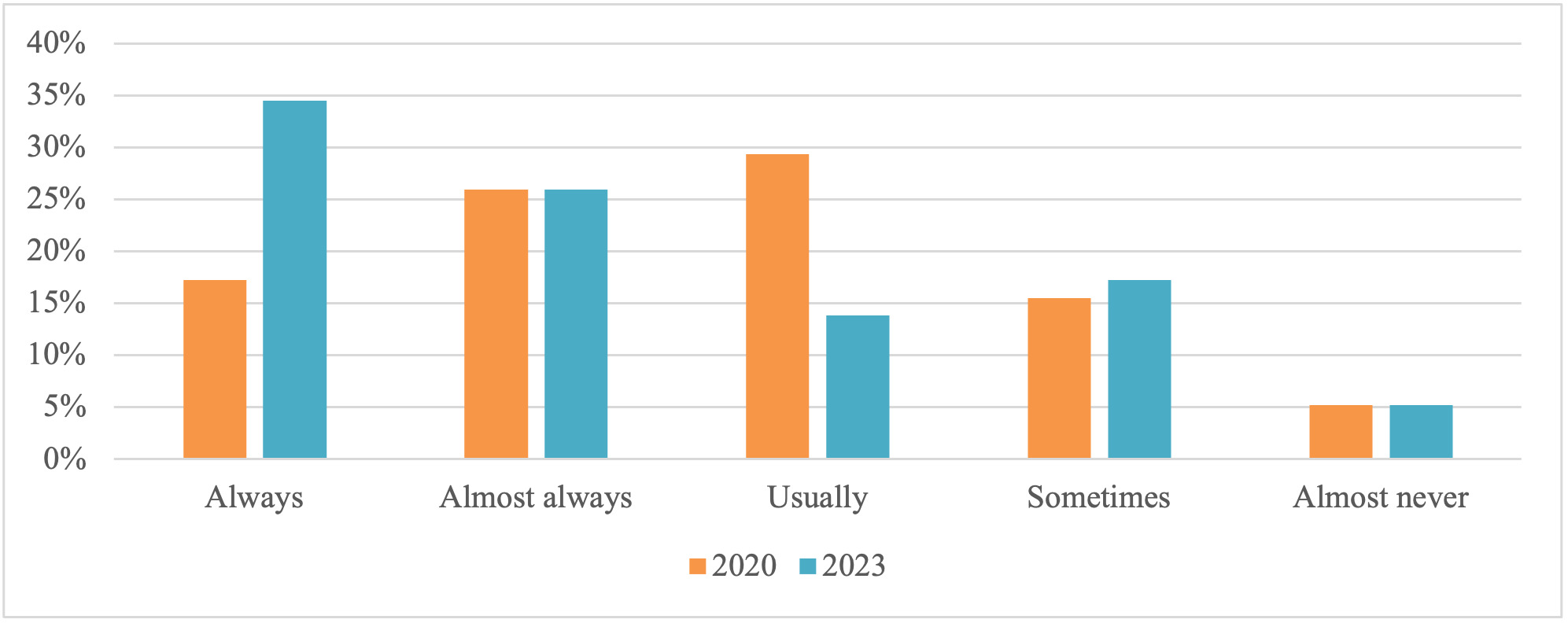
Health professionals reported including an assessment of the child’s transport needs during an initial assessment, ‘almost always’ (n=33, 26.2%) or ‘always’ (n=29, 23.0%). Only 11 health professionals (8.7%) ‘almost never’ included an assessment of transport needs, with the remaining respondents reporting ‘usually’ (n=20, 15.9%) or ‘sometimes’ (n=33, 26.2%). Repeat participants reported a significant increase in the frequency of transport needs being included in an initial assessment (Z = -3.54, p < 0.01; Figure 2).
Special purpose child restraints were the most prescribed or recommended solution (n=96, 76.2%), followed by standard ‘off the shelf’ child restraints or booster seats (n=92, 73.0%). Health professionals (n=39, 30.9%), who prescribed/recommended a specialty harness or vest often did so in conjunction with other seating supports, including standard child restraints (n=21, 53.8%), booster seats (n=20, 51.3%), special purpose child restraints (n=15, 38.5%) and booster cushions (n=6, 15.4%). Table 1 shows the change in 2023 compared to 2020 for repeat participant health professionals who were significantly less likely to recommend or prescribe a harness and, more likely to prescribe/recommend Australian standard car restraints or booster seats.
Among health professionals who had prescribed a special purpose child restraint under the National Disability Insurance Scheme (NDIS) funding system (n=79), there was a wide variation in the waiting time between identification of need and receipt of the restraint. The most common response among health professionals was that the process took 3-4 months (n=18, 22.8%), followed by: 1-2 months (n=10, 12.7%), 2-3 months (n=10, 12.7%), 4-5 months (n=8, 10.1%); 8-9 months (n=6, 7.6%), 5-6 months, 6-7 months (n=4, 5.1%), and 1-2 years (n=4, 5.1%). All other responses accounted for less than 5 percent of the sample (n=3). Five health professionals reported recommending a special purpose child restraint, but that funding was not approved. Repeat participant responses showed that compared to 2020, there were significant reductions (3-5 months to 1-2 months; Z = -6.28, p < 0.01) in the wait time to receive a special purpose child restraint in 2023.
In cases where a special purpose child restraint had been prescribed and obtained (n=113, 89.6%), the fitter was most often the supplier (n=63, 55.8%), followed by the prescribing health professional (n=17, 15.0%). Other fitters included the parent or guardian (n=9, 8.0%), mainstream car seat fitter (n=9, 8.0%), and 13 (11.5%) participants were not sure who fitted the child restraint system. Repeat participant responses showed an increase in the use of suppliers for fitting special purpose child restraints (Z = 5.10, p < 0.01).
After the initial prescription or recommendation of a child restraint system, there was variation in how frequently health professionals reviewed children’s transport needs. Approximately one third (n=38, 32.2%) conducted a review every 6-12 months, with most others doing so more frequently (1-3 months, n=22, 18.6%; 3-6 months, n=25, 21.2%). Only ten health professionals (8.5%) reported conducting transport reviews more than 12 months apart, and 13 (11.0%) reported they had never conducted a review. Eight health professionals did not complete this question. Repeat participants reported a significant increase in the frequency of reviews since 2020 (Z = 5.64, p < 0.01). The same number of participants reviewed every 6-12 months (n=18), however, there was a small increase (n=3) in the number of health professionals who reviewed transport needs every 1-3 months (n=3) and at least every month (n=4).
For health professionals with clients who transition to adult services (n=47), almost three quarters (n=35, 74.4%) include information relating to the client’s car seating and transport needs to the new service provider. For the 12 repeat participants, there was no change in their practice (X2 = 0.00, p = 1.00). Descriptive comparisons between the full 2020 and 2023 samples however suggest that there may be a small increase (6.4%) in the number of health professionals who included a handover of the child’s transport needs (2020 sample: 68% including handover). Health professionals reported a range of methods for providing this handover, including written reports and plans, verbal or email handovers with the new health professional(s), and provision of information to the family.
Health professionals’ knowledge and beliefs
All participants strongly agreed that children with disabilities and medical conditions have the same rights as other children to safe transport (Median=10, IQR = 0). All health professionals also reported having some knowledge and skill in addressing car seat travel needs for children with a disability or medical condition (considerable, n=20; 15.9%; some, n=81; 64.3%; a little, n=25, 19.8%).
Repeat participants reported a significant increase in their self-perceived knowledge and skill in addressing the car seating and transport needs of children with disabilities (Z = -6.61, p < 0.01). The proportion of health professionals with only a little knowledge/skill decreased (by 11.6%), while the proportion some knowledge/skill increased (by 17.9%).
Health professionals rated their confidence in their knowledge of a range of transport-related topics. The topic with the highest rated level of confidence was knowledge of road laws relating to transporting a child without a disability (MDN=7, IQR = 3) or with a disability (MDN=6, IQR = 3) in their own state or territory. Lower ratings were reported for knowledge of such laws in other states or territories, with a higher level of knowledge reported for children without disabilities (MDN=5, IQR = 4), than those with (MDN=3, IQR = 4). For repeat participants, there was a significant increase in perceived knowledge relating to: where to access information on car seating and transport options (2023 MDN=8, 2020 MDN=5; Z = -5.07, p < 0.01); non-specialist car seats that are still suitable for children with disabilities or medical conditions (2023 MDN=6, 2020 MDN=5; Z = -3.71, p < 0.01); special purpose car seats (2023 MDN=6, 2020 MDN=5; Z = -3.36, p < 0.01); compatibility of special purpose car seats with different vehicles (2023 MDN=5, 2020 MDN=3; Z = -3.44, p < 0.01). However, there were no increases in knowledge of accessories used for transport (2023 MDN=5, 2020 MDN=4; Z = -1.72, p = 0.08). Additionally, there was a significant increase (Z = -3.88, p < 0.01) in the confidence of transport law knowledge relevant to children with disabilities from 2020 (MDN=5, IQR = 4) and 2023 (MDN=6.5, IQR = 3).
Health professionals rated their confidence on topics related to the standard ‘Australian/New Zealand standard AS/NZS 4370:2013 Restraint of Children with Disabilities, or Medical Conditions, in Motor Vehicles’ and were only moderately confident in their knowledge of the standard (MDN=5, IQR = 4), and their application of the process outlined in this standard (MDN=5, IQR = 3). Only half of health professionals (n=64, 50.8%) reported having access to AS/NZS 4370:2013. Repeat participants reported significant increases in confidence in knowledge of responsibilities (Z = -4.248, p < 0.01), of AS/NZS 4370:2013 (Z = -3.36, p < 0.01) and their confidence in applying the standard (Z = -3.19, p < 0.01).
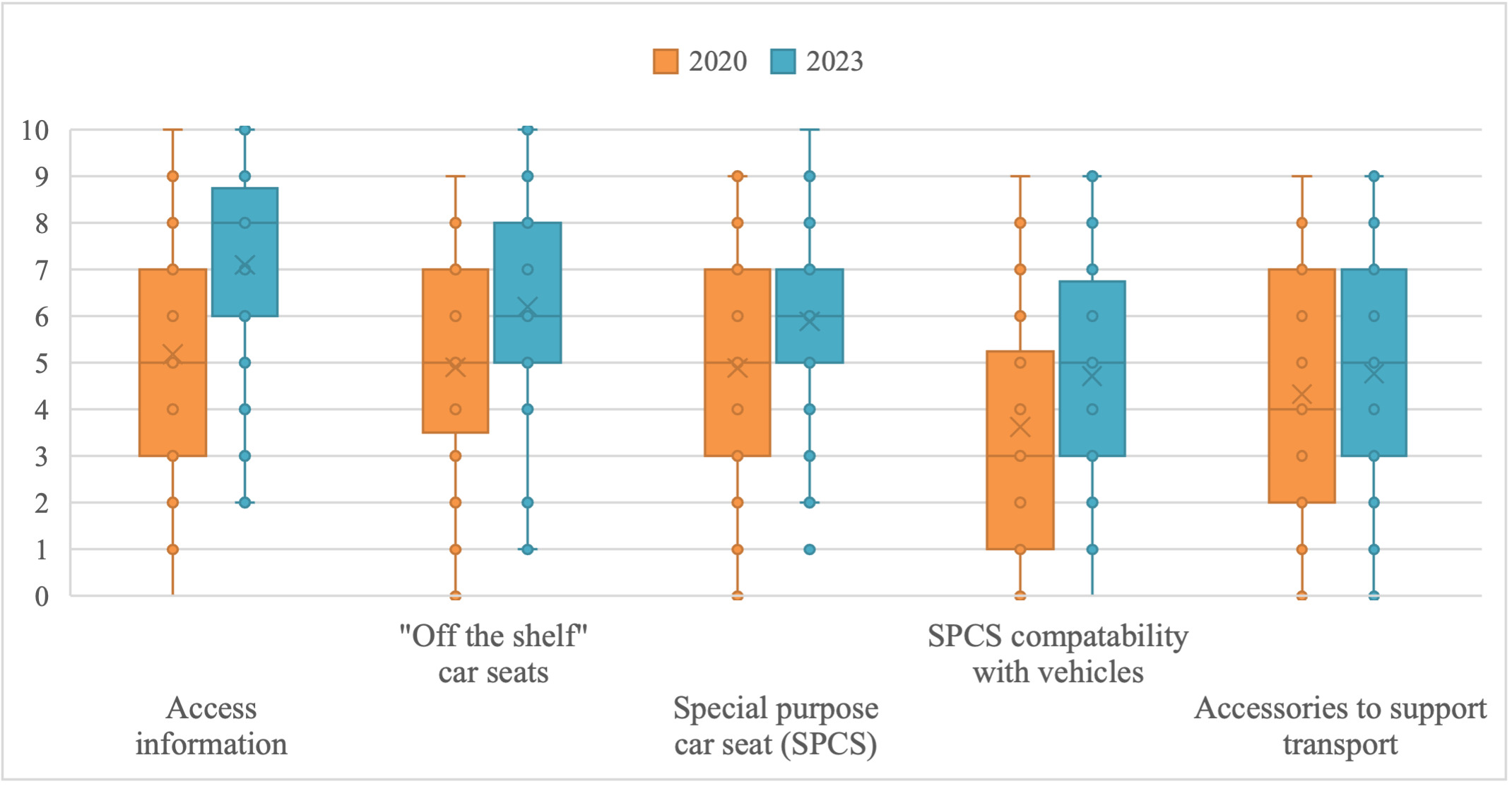
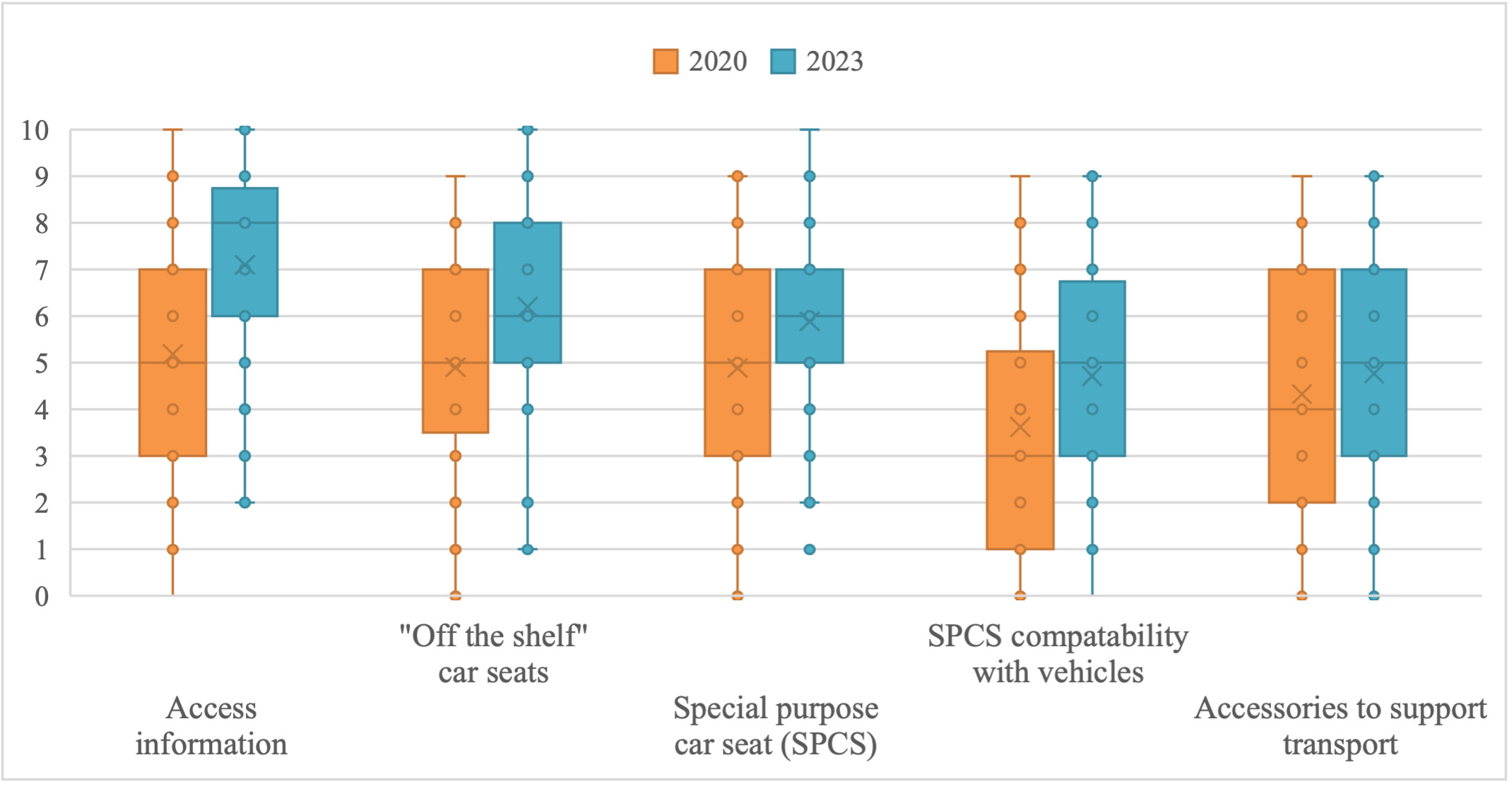
In relation to specific car seating products, health professionals were quite confident (MDN=8, IQR = 4) about how to access information about car seating options. In regard to specific products, they were most confident in their knowledge of standard ‘off the shelf’ seating options (MDN=6, IQR = 4); and special purpose child restraints (MDN=6, IQR = 3); but less confident in their knowledge of the compatibility of special purpose child restraints with different vehicles (MDN=5, IQR = 4); and of accessories for special purpose child restraints (MDN=5, IQR = 4). As shown in Figure 3, repeat participants reported a significant increase in confidence to find information about specific products (Z = -5.07, p < 0.01), knowledge of standard ‘off the shelf’ child restraints (Z = -3.71, p < 0.01), knowledge of special purpose child restraints (Z = -3.36, p < 0.01) and knowledge of the compatibility of special purpose child restraints with vehicles (Z = -3.44, p < 0.01). The change in confidence in relation to accessories was not significant among repeat participants (Z = -1.72, p = 0.08).
Challenges in addressing seating needs
Almost all health professionals (n=117, 92.9%) reported facing challenges when recommending or prescribing car seating for children with disabilities and medical conditions. The only challenge reported by more than half of health professionals in 2023 was finding restraint or seating that adequately meets the child’s head and body support needs (n=62, 53.0%). Other frequently reported challenges were the child travels in more than one kind of vehicle (n=55, 47.0%); multiple car seats are needed, and funding is only available for one seat (n=54, 46.2%); and the professional’s lack of specialised knowledge in this area (n=48, 41.0%). Other challenges that were less frequently reported include understanding vehicle requirements for restraints/seating, no clear process for ongoing review of the child’s seating needs/prescribed equipment, and the professional’s lack of specialised knowledge in this area. For repeat participants (n=52), there was not a significant increase in the number who experienced challenges (Table 2).
Accessing information
When asked how they developed their skills and knowledge to address car seat and travel needs for children with disabilities and medical conditions, health professionals most frequently reported learning from other health professionals (n=109, 86.5%). Other common sources of information included suppliers of special purpose child restraints (n=99, 78.6%), standards and guidelines (n=89, 70.6%), short courses and professional development (n=62, 49.2%), and online learning (n=62, 49.2%). Repeat participants reported increases in engagement in short courses and professional development (22%) (X2 = 4.00, p = 0.04), learning from suppliers of special purpose child restraints (14.4%) (X2 = 1.79, p = 0.18), and online learning (27.2%) (X2 = 11.53, p < 0.01). The least frequently reported source at both time points was through tertiary studies (2023: n=2, 1.6%; 2020: n=1, 1.9%).
Health professionals were also specifically asked if they had accessed a range of MACA resources, and if so, to rate how helpful they considered the information. The most accessed resources were the MACA website (n=114, 96.1%) and online training (n=66, 54.1%). Of the health professionals who accessed MACA resources, most reported the information was ‘helpful’ or ‘very helpful’ while information accessed through social media was rated ‘neutral’ for helpfulness. The MACA information sources rated as ‘very helpful’ were: website (n=82, 71.9%), online training (n=57, 86.3%), email support (n=27, 75%), phone support (n=28, 71.7%), social media (n=4, 36.3%). Most respondents learned about resources via the MACA website (n=66, 52.4%) followed by word of mouth (n=37, 29.4%). In addition to their own use, health professionals were asked to identify the most accessible sources of information for parents and caregivers on safely transporting children with disabilities and medical conditions. Comparing repeat participants across 2020 and 2023 timepoints indicates no differences across time. The most reported sources were allied health professionals (n=109, 86.5%; X2 = 0.56, p = 0.45) and websites (n=94, 74.6%; X2 = 0.24, p = 0.63), followed by in-person disability equipment suppliers (n=64, 50.8%; X2 = 2.56, p = 0.11), in-person mainstream shop (n=48, 38.1%; X2 = 0.50, p = 0.48), and social media (n=38, 30.2%; X2 = 0.05, p = 0.83). Other service providers, such as early childhood services (n=24, 19%; X2 = 0.07, p = 0.79), schools (n=22, 17.5%; X2 = 0.00, p = 1.00) maternal and child health services (n=19, 15.1%; X2 = 0.31, p = 0.58), and doctors (n=18, 14.3%; X2 = 1.13, p = 0.29) were less frequently selected.
Organisation knowledge and beliefs
All but one organisational representative (n=39, 97.5%) agreed that children with disabilities or medical conditions have the same rights as other children to safe transport (overall median=10, IQR = 0). Three-quarters of respondents reported that they were aware of the Conventions on the Rights of the Child (n=30, 75%) and the Convention on the Rights of Persons with Disabilities (n=30, 75%). There were no significant differences over time within the repeat participants (X2 = 0.00, p = 1.00; X2 = 0.50, p = 0.50 respectively).
The majority (n=38, 95.0%) of organisational representatives reported being aware of restraints made specifically for children with disabilities (special purpose child restraints). Most respondents (n=35, 87.5%) also reported being aware of the Australian/New Zealand standard (AS/NZS 4370:2013) relevant to car seating for children with disabilities or medical conditions. Almost all respondents (n=39, 97.5%) reported being aware of the road laws relating to travelling in a motor vehicle with children without disabilities in their state or territory. However, fewer respondents (n=30, 75.0%) were aware of road laws specific to travelling with children with disabilities or medical conditions. For repeat participants, there was a significant increase in the awareness of AS/NZS 4370:2013 (45.1%, X2 = 4.17, p = 0.03).
When comparing the full 2020 and 2023 samples, the results suggest an overall improvement across several areas. In 2020, most organisational representatives were aware of special purpose child restraints (85.2%) and AS/NZS 4370:2013 (67.2%). Knowledge of road laws for children with disabilities and medical conditions was also higher in 2023 than in 2020, both within (2020, 88.5%) and outside (2020, 60.8%) the organisation.
Of the 32 respondents whose organisations had an organisational strategy or plan, 12 (40%) had strategies or plans for safe transport of children with disabilities and medical conditions, 10 (33%) did not, and the remaining 10 respondents (33%) were unsure. When asked if their organisation had conducted research or activities to support the safe transport of children with disabilities or medical conditions, 16 (42.1%) said yes, 14 (36.8%) said no, and eight (21.1%) were unsure. Two participants did not respond and repeat participants did not show any significant change over time (11.1%, X2 = 0.25, p = 0.62).
Organisational representatives reported that multiple agencies (mean=4.4, SD = 1.4) were responsible for ensuring that the transportation needs of children with disabilities and medical conditions were met (Table 3). There was a significant increase in repeat participants who reported that both the state and Commonwealth governments were responsible.
Accessing information for organisations
Organisational representatives were also asked about MACA resources. Of the 26 (65.0%) participants who had accessed at least one MACA resource, the most common way they learned about them was online or via website (n=8, 30.8%), and word of mouth (n=5, 19.2%). The most accessed resources were the MACA website (n=20, 76.9%), social media (n=13, 50.0%) and online training (n=11, 42.3%). Both the email and phone services were accessed by seven (26.9%) organisational representatives. The most common rating of helpfulness for all resources was ‘very helpful’ (n=29, 50.0%), followed by ‘neutral’ (n=14, 24.1%). Seventeen organisational representatives (42.5%) reported referring others to MACA’s resources. Just over half (n=21, 52.5%) reported being aware of MACA’s online training, and a similar number (n=26, 65.0%) reported being interested in the training. However, several participants noted that the cost was a barrier to participating in the training.
Discussion
This study provides a comprehensive overview of the perspectives and experiences of health professionals and organisational representatives regarding the transport of children with disabilities and medical conditions. It also offers a comparison with the findings from 2020, as reported in Black et al. (2024), and identifies the usefulness of increased educational resources provided by MACA. The results indicate significant progress in several areas over the past four years, highlighting the evolving practices and increased resources available to support the transport needs of children with a disability or medical condition.
A key finding of this research is the significant increase in the frequency with which health professionals include transport needs in their initial assessments of children with disabilities and medical conditions. These professionals are now significantly more likely to conduct regular reviews of transport needs to accommodate children’s changing needs as they grow, compared to four years ago. While no causal links can be drawn, this shift in clinical practice has occurred over the same period that there has been an increase in online educational resources available. An important finding of this research is that the provision of online educational resources, including those offered by MACA, have proven to be both helpful and informative for health professionals. As caregivers have previously reported health professionals as being their preferred source of information about their child’s transport needs (Black et al., 2023), increased professional knowledge may also in turn improve caregiver knowledge, ability in confidence.
Another key finding of this study is the significant reduction in wait times for the receipt of special purpose child restraints. Among repeat participants, there were fewer reports of very short wait times (less than one month) compared to the 2020 data. However, common wait times also decreased from 5-6 months to 3-4 months, showing an overall improvement in consistency. Additionally, there were also fewer reports of waiting more than a year. This reduction in wait times is likely linked to the increased focus on transport needs during initial and review assessments, as well as the overall improvement in professionals’ knowledge and confidence across a range of relevant topics. This is an important change because long wait times result in a lack of appropriate supports and reliance on modifications, decreasing participation for children and families in everyday activities (Black et al., 2024). Providing families with appropriate equipment that meets the needs of their child decreases the likelihood of injury or death in the event of a crash, as well as decreasing the use of modifications that do not meet the legislative requirements and have not been crash tested (Cook, Brown, et al., 2024; Cook, Whyte, et al., 2024).
Despite these positive developments, the study also highlights areas where further improvements are needed. Although reports of some challenges have substantially decreased (e.g., navigating documentation processes, securing funding for prescribed equipment, lack of appropriate training and professional support), other challenges persist. Notably, an increase in the difficulty of understanding vehicle requirements for restraints and seating, as well as challenges with height and weight restrictions. Further efforts to increase health professionals’ knowledge regarding these requirements are needed to address this barrier in clinical practice. The development of future educational resources providing health professionals with more information about different vehicle types, as well as height, weight, or size restrictions of products would improve efficiency and efficacy in the prescription of restraints and seating for children with disabilities and medical conditions.
The findings also point to the need for more research to inform the development of more inclusive and equitable policies, standards, and laws. This will provide clarity about roles and responsibilities, affording children with disability the safety protections necessary when travelling in motor vehicles, equal to other children in the community. Currently, a wide range of agencies are responsible for the safe transport of children with disabilities and medical conditions, including Commonwealth and state/territory governments, the NDIS, and transport agencies/regulators. Effective coordination and communication among these agencies, supported by rigorous evidence, are essential to address the unique transportation needs of children with disabilities. Other issues, such as the cost and availability of appropriate equipment, also remain challenges that must be addressed by relevant institutional bodies.
Strengths and limitations
This study contributes new knowledge to an area of practice with limited previous research. The strengths of this study include its national scope and subgroup of repeat participants, which enabled an assessment of change over time among experienced professionals. However, as noted above, the repeat participant subgroup is susceptible to selection bias which may limit the representativeness of the total sample.
Several limitations should be noted. First, as with all self-report surveys, it is unknown whether responses accurately represent participants’ actual experiences, knowledge, beliefs and behaviour. Observational or similar studies, such as those employed by Yonkman et al. (2010), could provide a more objective assessment of practice. Comparison between the 2020 and 2023 data was based on a small number of repeat participants to reduce variability unrelated to time. This approach may introduce bias, and small sample sizes for some questions could limit detection of significant changes. Repeat participants may be more engaged in the field and content, potentially overestimating improvements. Finally, focusing on health professionals and organisational representatives may not fully capture the experiences of all professionals working with children with disabilities and medical conditions.
Conclusion
This study provides some promising indications that progress has been made in the transport of children with disabilities and medical conditions over the past four years in Australia. Key findings based on our data show a significant increase in the frequency of transport needs included in initial assessments and subsequent reviews by health professionals, as well as a significant reduction in wait times for special purpose child restraints. Our findings point to the potential importance of educational resources and training, such as those offered by MACA, in enhancing the knowledge and skills of healthcare professionals, which may promote road safety outcomes for children with disabilities and medical conditions. However, despite these advances, significant challenges must be addressed to further improve the safety and accessibility of transport for children with disabilities and medical conditions. A more consistent and evidence-based approach is required across all jurisdictions to ensure that every child has access to safe and appropriate transport solutions. Considering these findings, it is imperative that regulators, researchers, health professionals, industry, policymakers, and not-for-profits continue to collaborate to enhance equitable road safety for children with disabilities and medical conditions.
AI tools
AI tools were not used in this study nor in the preparation of this paper
Author contributions
Emily D’Arcy: Conception, Design, Execution, Analyses, Writing Original Draft, Writing Critical Revision. Melissa H. Black: Conception, Design, Writing Original Draft, Writing Critical Revision. Maya Hayden-Evans: Conception, Design, Execution, Writing Original Draft, Writing Critical Revision. Sarah McGarry: Design, Execution, Writing Original Draft, Writing Critical Revision. Helen Lindner: Conception, Design, Writing Original Draft, Writing Critical Revision. Emma Clarkson: Conception, Design, Writing Original Draft, Writing Critical Revision. Stuart M. Chesher: Analyses, Writing Original Draft, Writing Critical Revision. Torbjorn Falkmer: Conception, Design, Writing Original Draft, Writing Critical Revision. Kevin Netto: Analyses, Writing Original Draft, Writing Critical Revision.
All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by Mobility and Accessibility for Children in Australia Ltd and funded by the Australian Government Department of Social Services (grant number RES-62630). The sponsors have supported the research with input to study design, collection, analysis and interpretation of data; manuscript preparation and the decision to submit the manuscript for publication.
Ethics approval
Ethical approval for this study was obtained from the Curtin University Human Research Ethics Committee (HREC number HRE2020-0257) on 22 May 2022.
Data availability statement
De-identified data from this study can be made available via a direct request to the corresponding author.
Conflicts of interest
Helen Lindner and Emma Clarkson are co-founders of MACA. Lindner additionally serves as CEO, and Clarkson serves as Director of MACA. Kevin Netto sits on the MACA board. These relationships had no influence on the research or its findings.