


Introduction
Background
The previous decade 2011-2020, was named Decade of Action for Road Safety by the United Nations Organization (UN). UN expected to save about 5 million lives from global road traffic crash (RTC) fatalities during this decade.[1] However, over 1.19 million people still lose their lives to RTC annually and it is the leading cause of death for the age group 5-29 years old (WHO, 2023). It is important to highlight that 92% of total RTC-related deaths occurs in low and middle-income countries, even though they have around 60% of total global vehicles (WHO, 2023).
The causes of RTC may be categorised in several ways including: mechanical failure of the vehicles (Hoque & Hasan, 2007), weather conditions (Sabir, 2011), road design and road environment factors (Cheng & Washington, 2008), and driver behaviour (Zia et al., 2014). There is rich literature available on all of these aspects of RTC. However, most of the research studies on RTC are based on microdata of developed countries (e.g., Hoque & Hasan, 2007; Sabir, 2011). By microdata, we mean the level of details with which the RTC are recorded. In developed countries, reported micro level crash data include the type of crash, parties involved in road crashes, the details about each party (e.g., driver or passenger, seating position, age, gender, details of the other party or object involved), the details about vehicles (e.g., make/model, year of manufacturing, if it was insured), contributing crash factors (e.g., road condition, weather) (Sabir, 2011). All these details make RTC data rich and suitable for identifying the causes of road crashes. Furthermore, in high-income countries, RTC data are available for research purposes. However, in low- and middle-income countries (such as Pakistan), data at such detail are not available nor easy to access and analyse for research and therefore not explored (Zia et al., 2014).
The Safe System approach is another aspect of enhancing road safety and moving towards “vision zero” that emerged from the UN Decade of Action. Based on the approaches from Sweden and the Netherlands, Australia was the first country to adopt the Safe System in the national road safety strategy (ATC, 2011). The Safe System is based on a multilayer of protection, that aims to reduce the risks of crashes and also minimise the harm to involved parties in RTC (DOT, 2022). Furthermore, it is a holistic approach to reducing road safety and a deviation from the traditional approach because it focuses on both human mistakes and vulnerabilities while focusing on designing systems that have protections for everyone. There is less adaptation of the Safe System to reduce RTC in low- and middle-income countries in general and Pakistan in particular. The current study is a contribution to the existing literature on RTC of low- and middle-income countries.
This study focused on the nexus between RTC and Ramadan including the health and social risk factors. Factors included were health (due to fasting) and social factors (e.g., driver carelessness) to rank various criteria (reaction time, cognitive responses, body efficiency, and anxiety) that may contribute to RTC during Ramadan. The study contributes to the literature in several ways. First, it adopts a fuzzy approach incorporated with multi-criteria analysis models (Technique for Order Preference by Similarity to an Ideal Solution (TOPSIS)) to overcome the absence of micro-level crash data in Pakistan. Secondly, it considers fasting as one factor that may affect the RTC risk. Thirdly, the study ranks reaction time, cognitive responses, body efficiency, and anxiety to identify the major contributing factors to RTC in Ramadan. Finally, the approach adopted in the study could be replicated in any low- or middle-income country where there is an absence of detailed micro-level RTC data to identify various RTC risk factors for improving road safety. The study also highlights the Safe System approach for reducing RTC in Pakistan.
Literature review
RTC is an important area of scholarly research and there is an abundance of research investigating contemporary issues. However, the literature review focused on the contributing factors in RTC during the holy month of Ramadan.
Ramadan is a fundamental element of Islam. Muslims observe fasting during the month of Ramadan. Medical literature reports various positive (Reilly & Waterhouse, 2007) and negative impacts of fasting on the human body (Halawa, 2020). On the positive side, fasting may improve health by reducing bad cholesterol and weight (Reilly & Waterhouse, 2007). On the other hand, the negative impacts of fasting can be more severe when Ramadan occurs during summer when the temperature is higher and the number of daylight hours, and therefore the number of fasting hours, is longer (Tolon & Chernoff, 2007). Fasting can decrease alertness and mood (Roky et al., 2000), increase driver distraction (Ferreira et al., 2009), and influence energy balance, psychosomatic conditions, drug compliance, with the effects more severe for people with major or minor health complications (Leiper & Molla, 2003). Fasting also prohibits drinking and can cause issues from dehydration (Leiper & Molla, 2003), which include: delays in reaction time and performance levels (Kempton et al., 2011). Similarly, sleep can be disturbed during Ramadan (Roky et al., 2001). Similarly, Ramadan can affect sleep quality (BaHammam, 2005). As sleep quality decreases, this can negatively impact human psychomotor performance, alertness and physical performance (Roky et al., 2004). Solianik et al. (2016) reported an increase in anger with longer fasting duration. Furthermore, during the fasting period, Muslims abstain from smoking. Smoking deprivation can decrease the driver’s cognitive responses (Havermans et al., 2003). These negative impacts of fasting combined with behavioural aspects such as speeding may increase RTC risk during Ramadan (Taylor & Dorn, 2006).
The existing scholarly literature on Ramadan and RTC nexus mainly discusses RTC-related statistics and compares Ramadan and non-Ramadan months using data from hospitals, rescue services, or observing traffic on a limited section of roads. Several studies reported an increase in road crashes during Ramadan (Al-Houqani et al., 2013; Gulek, 2024; Kalafat et al., 2016; Mehmood et al., 2015; Mohseni & Molla, 2017; Tahir et al., 2013; Tolon & Chernoff, 2007).
Kalafat et al. (2016) found a higher number of serious crashes, resulting in fatalities and injuries, during Ramadan compared to a non-Ramadan month in Turkey in 2011. In a study in Pakistan, Mehmood et al. (2015) analysed data from two hospitals in Karachi city from 2006-2011 and reported an increase in road crashes with most vulnerable road users, motorcyclists and pedestrians, most affected during Ramadan. Similar findings were reported by Tahir, et al. (2013) for 35 districts of Punjab province (Pakistan) using Rescue 1122 data from 2011. Tahir et al. (2013) also reported more crashes during Ramadan, particularly in evening peak hours, with motorcyclists involved in most of the crashes (about 60%). Other studies that used hospital data reported increased RTC during Ramadan in the United Arab Emirates (Al-Ain city) (Al-Houqani et al., 2013) and in Iran (Kermanshah) (Mohseni & Molla, 2017).
Gulek (2024) quantified the effects of fasting on the RTC for provinces of Turkey that observe more fasting and reported a 25 percent increase in the probability of RTC due to fasting. The finding of the impact of fasting on RTC is smaller than driving while impaired by drugs but more prominent than with mild sleep deprivation (Gulek, 2024). Similarly, Al-Masaeid et al. (2020) investigated the traffic level on twelve urban major arterial segments, in Amman, Jordan for the period 2013-2017 and reported that while the traffic level was similar in Ramadan and non-Ramadan months, there was a significant increase in RTC during Ramadan.
However, other research has reported little or no impact of Ramadan on traffic or RTC. For instance, in Turkey, Yıldırım-Yenier et al. (2016) reported no changes in drivers’ honking, speeding or seat belt use during Ramadan month compared to a non-Ramadan month. Similarly, in Semey, East Kazakhstan, Tlemissov et al. (2017) reported a lower number of injuries among older people (over 60 years) during Ramadan. However, these studies were not directly linked with RTC, as Yıldırım-Yenier et al. (2016) focused on traffic flow and associated characteristics and Tlemissov et al. (2017) focused all injuries for older people not just RTC-related injuries. While Khammash and Al-Shouha (2006) reported no changes in RTC for Jordan during Ramadan of 2004, compared to the subsequent month of the same year, their study was based on limited data (two months from one hospital emergency department).
In a nutshell, some studies have examined RTC during Ramadan using RTC data from hospitals (Mehmood et al., 2015), emergency services (Tahir et al., 2013) or limited region surveys (Yıldırım-Yenier et al., 2016). While these studies and data are helpful, they provide limited insights into road crashes during Ramadan and do not consider how RTC are impacted by the physical experience of fasting drivers.
To address this knowledge gap, in this study we employed MCDM-based techniques (Batool et al., 2018; Zia et al., 2014). These studies were based on analysing RTC in Pakistan using police-recorded road crashes. Pakistan police recorded RTC data are mostly handwritten, descriptive narratives with varied levels of detail. Analysis would require a herculean, manual review to identify every RTC that occurred during Ramadan (Zia et al., 2014). The MCDM-based approach takes a different approach by engaging professionals (i.e., health workers and transport experts) to identify and weigh the factors that could contribute to RTC during Ramadan. Furthermore, the study ranks various factors associated with Ramadan that may contribute to more RTC during Ramadan. This ranking of relevant factors creates new dimensions of the Ramadan and RTC nexus. Finally, the applied MCDM-based approach can be adopted in any other country or region to identify and rank the most critical factors causing RTC during Ramadan.
Study setting
Pakistan is a developing country with a population of over 242 million (MoF, 2024). It has over 14,480 km of highways and motorways (MoF, 2024). Accordingly, there are about 135 vehicles per 1,000 inhabitants of Pakistan (PBS, 2018).[2] The rate of motorisation is on the rise (Table 1) due to rising per capita income, lower interest rates, and the introduction of new automobile manufacturing firms due to the implementation of the automobile policy 2016-21 (MoF, 2021).
But the road safety situation in Pakistan is dismal. In 2019, 10,429 RTC were reported, including about 4,772 fatal RTC, reporting 5,816 fatalities and 12,886 injuries (PBS, 2020). We note that the RTC may be underreported because there is no proper RTC recording mechanism in Pakistan; instead, the RTCs are recorded by police like any other crime (Zia et al., 2014). The absence of detailed data on RTC in Pakistan makes it difficult to conduct extensive scholarly work on RTCs using traditional econometric tools like those used in road safety studies in high-income countries (Claus & Warlop, 2022; Tscharaktschiew, 2020; Tyndall, 2024; Van Ommeren et al., 2013).
The official reported numbers of RTC in Pakistan, show an increasing trend despite underreporting (Table 1). The motorway police for motorways and national highways (excluding urban and local roads) keep separate records of RTC in their jurisdiction. The motorway police data show a mixed trend of road crashes during the 2015-2020 period (Table 2). According to motorway police, the three notable causes of road crashes on motorways are driver carelessness (H. Al-Masaeid, 2009; Zia et al., 2014), dozing at the wheel (Bioulac et al., 2017; Shah & Khattak, 2013), and tyre bursting (Hoque & Hasan, 2007; Shah & Khattak, 2013). While tyre bursts could be included in mechanical failure, in low- and middle-income countries, including Pakistan, no special attention is given to vehicle fitness or proper checking of vehicles before long routes, this could also be categorised as driver carelessness (Hoque & Hasan, 2007). Both driver carelessness and fatigue may be influenced by the fasting period during Ramadan.
Pakistan is a Muslim-majority country. In the month of Ramadan, Muslims observe fasting and abstain from any intake (i.e., eating, drinking, smoking) from sunrise (Suhur) to sunset (Iftar). It may have substantial implications for drivers, especially in areas where Ramadan occurs during summer with more daylight hours e.g., from 2008-2019, Ramadan occurred between May and August).[3] During these warmer and longer days, drivers may experience health issues like dehydration, hunger or fatigue related to getting up early for fasting and shorter summer nights. Additional factors may also contribute to RTC during Ramadan including: speeding on approach to sunset (reaching a destination for Iftar) or negative physical reactions related to not smoking. All these factors may influence a driver’s reaction times and alertness, which may affect the number of RTC (Ferreira et al., 2009; Roky et al., 2000).
The initial study aim was to identify and rank risk factors (health and social) associated with RTC while considering the impact of Ramadan in summer days. However, due to the absence of official micro crash data, such analyses were not possible. Therefore, this study used an MCDM-based TOPSIS approach to study the risk factors contributing to RTC in Pakistan during Ramadan. TOPSIS is simple to apply, and it does not need extensive data like popular approaches (e.g., econometric modelling or simulations) used in the scholarly literature on RTC.
Method
The objective of this work was to identify and rank the crash risk factors during Ramadan. However, as no detailed crash data are available in Pakistan, there are several methodologies within the domain of multi-criteria decision-making (MCDM) models that could be adopted to rank Ramadan-related RTC risk factors. These include the Analytic Hierarchy Process (AHP) (Ali et al., 2018; Sabir et al., 2018), the Technique for Order Preference by Similarity to Ideal Solution (TOPSIS) (Sabir et al., 2020, 2022), and VIKOR (ViseKriterijumska Optimizacija I Kompromisno Resenje, meaning Multicriteria Optimisation and Compromise Solution in Serbian) (Ali, Razi, et al., 2019). TOPSIS was the preferred option due to its simplicity in application, geometric clarity, ability to handle mixed criteria and less sensitivity to weight changes (Madanchian & Taherdoost, 2023).
The fuzzy set theory was introduced by Zadeh (1965) to address vagueness of information. Therefore, a better version of TOPSIS is fuzzy TOPSIS which can better handle information vagueness (Rehman & Ali, 2022). We employed the MCDM-based fuzzy TOPSIS model and developed the following theoretical framework.
The model shows two risk factors for RTC during Ramadan, namely, health factors related to fasting and social factors. As identified in the literature, these factors influence drivers’ reaction or response time, anxiety level, cognitive responses, and body efficiencies and may increase the likelihood of RTC. For this study, we characterised our alternatives into social factors and health factors in RTC during Ramadan. Social factors included driver carelessness (e.g., speeding, absent-mindedness etc), increase in the number of vehicles, and lack of training and licensing in drivers. It is important to highlight that carelessness is not just related to Ramadan (e.g., H. Al-Masaeid, 2009 reported a 22.5% increase in RTC due to driver carelessness), however, driver carelessness may increase during fasting. For studying health factors, we considered fasting conditions. Health factors included deprivation from addictions (e.g., smoking is prohibited during Ramadan), dehydration, sleeplessness, weather (e.g., extreme heat, foggy weather, etc), and lack of proper nutrition. Criteria include reaction/response time, anxiety, cognitive response, and human body efficiency. Figure 1 shows the alternatives and the relative criteria that were analysed.

Fuzzy TOPSIS
Fuzzy set theory
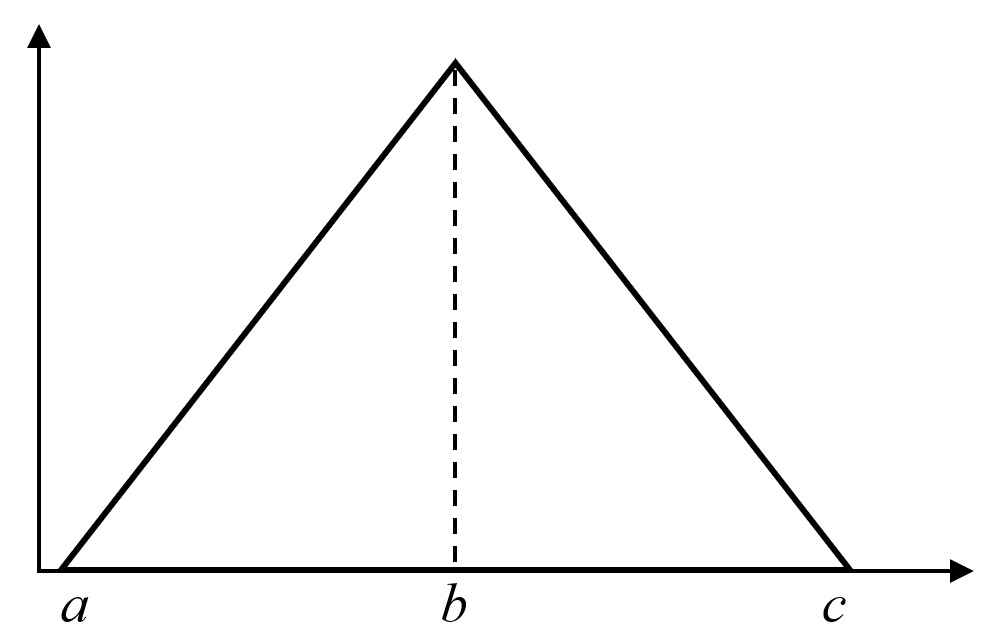
The fuzzy set theory (Zadeh, 1965) was developed to account for uncertainties and human imprecisions in data. The Triangular fuzzy numeric approach was adopted for this study, letting the triplet (a, b, c) define the fuzzy numbers (Figure 2).
Fuzzy set theory converts linguistic variables into mathematical representation on a five-point Likert scale of agreement (very low, low, moderate, high, very high.). Table 3 below shows the linguistic terms and their relative triangular fuzzy numeric numbers adopted from Afful-Dadzie et al. (2014).
Let  be the fuzzy set and its value lies between 0-1. Linguistic variables are converted into triangular fuzzy numeric numbers “” using the Equation (1) shown below.
μˆA={0, if x<a,x−ab−a if a≤x≤b,c−xc−b if b≤x≤c,0, if x>c
The fuzzy set theory is combined with MCDM which can deal with analysing a set of alternatives in complex decision-making scenarios (data contain uncertainties) by helping to assess different options based on multiple criteria. It involves ranking/prioritising the alternatives that are simultaneously evaluated based on multiple criteria.
TOPSIS
Yoon (1980) developed TOPSIS as a technique to measure the relative distance between positive and negative ideal solutions and selects alternatives based on those distances (Liang et al., 2018). This method is based on the idea that the best alternative should be closest to the ideal solution and farthest from the negative ideal solution. The study utilised fuzzy set theory combined with the TOPSIS approach to evaluate the influence of health and social factors on RTC during Ramadan. The rationale behind this technique is to consider the inherent ambiguity and subjectivity in expert assessments of parameters such as response speed, cognitive reaction, and anxiety. The fuzzy set helps to convert subjective evaluations into numerical fuzzy values, enabling a detailed examination of the impact of these factors on RTC. TOPSIS was employed to rank these aspects in a methodical manner, considering their proximity to an ideal solution. This approach integrates health and social factors into a unified framework, which accurately represents their collective impact on risks associated with RTC.
TOPSIS is one of the MCDM techniques, which focuses on analysing the alternatives based on criteria (Sen et al., 2016). TOPSIS technique has been used extensively in various fields, including forestry (Sabir et al., 2020), supply chain management (Ali et al., 2020), developing studies (Ali, Sabir, et al., 2019), and production management (Ali, Haroon, et al., 2019).
TOPSIS analysis is described in the following steps:
Step 1
The first step is the construction of a normalised decision matrix as per Equation (2). Matric = matrix where = alternatives and = criteria.
rij=xij∑x2iji=(1,2……m),j=(1,2…,n)
Where, is the score of the option for criteria
Step 2
In the next step, a weighted normalised decision matrix is constructed as shown in Equation (3), where is assigned weights for
vij=wj×rij
Step 3
In step 3, the ideal and negative ideal solutions are determined as per Equation (4) and Equation (5), respectively.
Ideal solution (A∗)A∗=(v∗i,…,v∗m)
Where
Negative Ideal Solution (A′)A′=(v′j,…,v′n)
Where
Step 4
This step calculates separation measures for alternatives as per Equation (6) and Equation (7)
Ideal Alternative (S∗i)S∗i=[∑(v∗i−vij)2]1/2
Negative Ideal Alternative S′[S′i=[∑(v′j−vij)2]1/2
Step 5
The second last step calculates relative closeness as per Equation (8)
C∗i=S′i(S∗i+S′i)
Where
Step 6
Finally, using calculated values of the ranking is made for alternatives. These values are set in descending order, and the highest value is the most important criteria/alternative, whereas the alternative associated with the lowest value shows the least important alternative.
Data
This study used primary data from two surveys because two different target experts’ responses on two different aspects of RTC are required for the TOPSIS method. The surveys were conducted during May 2021.
The first survey was health-related and focused on seeking feedback from health experts on the responses of the human body while fasting, especially during summer. These participants were targeted instead of the general public whose responses about the impact of fasting was considered too subjective. Respondents (n=46) were health care experts, the majority of respondents were doctors. Feedback was collected from various hospitals in Pakistan through an online survey using Google Forms. The first section of the survey was demographic information about the respondent (e.g., age, gender, profession). The second section of the survey was how the criteria (i.e., reaction time, cognitive responses, body efficiency, and anxiety) were impacted by fasting. Responses were recorded as per the scale in Table 3 (Afful-Dadzie et al., 2014).
The second survey focused on the social aspects of driving behaviour. Respondents (n=51) were mainly engineers and drivers. Again, the survey conducted using Google Forms and consisted of two sections with the first section being questions on respondent demographics. The second section of the health survey seeks responses from health experts on how they think that criteria such as reaction time, cognitive responses, body efficiency, and anxiety are influenced by smoking (or other addictions such as marijuana, sniffing or alcohol), sleeping disorders, lack of proper nutrition, dehydration, and weathering (the cumulative impact of chronic stress and social inequities on an individual’s health). The respondents were asked to give their feedback on how these criteria are influenced by driver carelessness, increasing number of vehicles on roads, and lack of proper driver training and licensing. The results of both these surveys were used in TOPSIS for further analysis.
Results and Discussion
Results of the TOPSIS method are presented in Table 4. The highest scored response was reaction time, followed by anxiety then cognitive response. At the same time, body efficiency scored the lowest. It implies that according to the experts, the most important factor influenced by fasting during Ramadan on RTC is reaction time.
Furthermore, fuzzified data from the survey were also used to construct a normalised matrix. After making the normalised matrix, the weighted normalised matrix was constructed by multiplying the fuzzy weights of the criteria with the normalised matrix. Finally, the relative distances of the criteria from the ideal and negative-ideal solutions were calculated. These solution values were then further used for calculating the relative closeness (Figure 3).
Fatigue due to disturbed or reduced sleep was identified as a major contributor that increased the rate of RTC, training and licensing were the second highest contributor with weather having the least effect. Interestingly, neither the number of vehicles nor nutrition were identified as critical factors in RTC in Pakistan during Ramadan.

Pakistan being a lower-middle income country (The World Bank Group, 2024), has many traffic-related issues. The road safety situation, in general, is not good. This study focused on the RTC during Ramadan. The result identified that slow reaction time is the major factor of fasting during Ramadan related to an increase in RTC. These findings are consistent with the earlier literature that reported slow reaction times during Ramadan (Kempton et al., 2011). Similarly, anxiety, cognitive responses, and body efficiency were ranked as the second, third and fourth most important factors for RTC in Ramadan. These findings are also consistent with studies as discussed in the literature review. However, this study shows that anxiety is more important than drivers’ cognitive response or body efficiency for increasing RTC risks during Ramadan. At the same time, cognitive response was ranked more important in the risk of RTC than body efficiency.
We note the relative closeness of the top three ranked factors (i.e., sleeplessness/dozing at the wheel, lack of proper training/licensing and carelessness). The finding of fatigue impacting RTC during Ramadan is consistent with previous research findings (Roky et al., 2001). Also, the highest factor impacting RTC on motorways in Pakistan is fatigue or dozing off the wheel. AlShareef (2021) also reported an increase in RTC due to sleeplessness. Ramadan can alter lifestyle, sleep patterns and quality, which can cause a change in individuals’ behaviour during the day (BaHammam, 2005). The second major factor in RTC in Ramadan was a lack of training and licensing. This is becoming a key issue in Pakistan with increasing per capita income where with easy access to car loaning facilities and a lack of formal vehicle driver training and licensing mechanisms, there is a larger number of underage drivers, untrained and unlicensed drivers. These factors are consistent with Hussain and Shi (2021). Strict policies regarding licensing and underage driving need to be imposed. There is a role for greater driver training towards licensing and government needs to create a formal system for this.
Carelessness was found to be the third highest contributing factor and included the condition of the car, driver distraction and speeding. Data extracted from motorway police (Table 2) show over half of RTC (53.6%) that occurred during the year 2015-2020 were attributed to driver carelessness toward the vehicle or the road. As already highlighted, carelessness is not limited to Ramadan. Driver carelessness is a major RTC cause in low- and middle-income countries (H. Al-Masaeid, 2009). We propose that driver carelessness adds to other factors to become more prominent during Ramadan. Secondly, Pakistan is a lower middle-income country and has an older vehicle fleet with little attention to vehicle roadworthiness and maintenance. Both the government and the individual have a role in maintaining a safe vehicle fleet. The government needs to implement policies to require people to ensure regular maintenance and roadworthy checks. Commercial and private drivers need to maintain their vehicles to minimise injuries in the event of a crash.
The impact of drivers’ urge for smoking was a greater factor in RTC during Ramadan than nutrition, dehydration, or vehicle numbers on the road. It is also noted that weather conditions had a lesser role in RTC during Ramadan compared to all other factors considered in this study.
Pakistan is a Muslim-majority country however, observing fasting during Ramadan is only compulsory for healthy Muslims. As per Islamic teachings, Muslims with medical issues can skip fasting or fast later for missed days. Given the majority of the population is young (67% under 30 years of age; PBS, n.d.), and therefore healthy, it is likely that most of the population observe fasting during Ramadan. Yet there is minimal caution about the potential negative impacts of fasting during the month of Ramadan. Given the impacts of fasting, particularly increased fatigue, and the importance of a Safe System, governments need to develop and implement policies to manage risks during the month of Ramadan.
Conclusion
This study used the MCDM-based TOPSIS method to identify and rank social and health factors associated with RTC during Ramadan using Pakistani data. The results indicate that lack of sleep, absences of licensing and driver carelessness are the three major sources of RTC during Ramadan. The study has various policy implications for policymakers, traffic police officials, parents and researchers. The study could help reduce RTC during Ramadan and contribute to the Safety System Approach of RTC that goes beyond the traditional RTC reduction approach.
Acknowledgements
The authors would like to thank the anonymous reviewers and the journal editorial team for suggesting useful feedback to improve the earlier version of this manuscript.
Author contributions
Yousaf Ali: idea, supervision, proof-reading. Ahmed Owais Durrani: data collection, write-up, analysis. Muhammad Sabir: literature review, write-up, analysis.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors
Ethics
The study was conducted using the protocols that were reviewed and approved by the Ghulam Ishaq Khan Institute of Engineering Sciences and Technology (Ref: F.No.Giki/SMgS/2023-1).
Data availability statement
The secondary data on the road accidents can be obtained from the Pakistan Bureau of Statistics website (https://www.pbs.gov.pk/). Due to the confidentiality clause, the primary data collected through surveys from drivers and health professionals cannot be publicly.
Conflicts of interest
The authors declare that there are no conflicts of interest.
The United Nations General Assembly Resolution 68/269.
Calculated as: Total registered vehicles were 30,757, 507 in 2019 (PBS, 2020), and the total population was 223 million in the same period. This makes it about 138 vehicles per 1,000 inhabitants.
As per Islam, Muslims observe fasting during the holy month of Ramadan. This is the fundamental element of Islamic basic five elements. Ramadan is the ninth month of the lunar calendar year, which is 12-13 days shorter than the Gregorian calendar year. Therefore, Ramadan completes a rotation after every thirty years. This means the month of Ramadan shifts each year.